What updates are presented in the IOC consensus statement on RED-S 2018?
Prevention
Awareness is the key to prevention, yet RED-S continues to go unrecognised. Less than 50% of clinicians, physiotherapists and coaches are reported as able to identify the components of the female athlete triad. In a survey of female exercisers in Australia, half were unaware that menstrual dysfunction impacts bone health. Note that these concerning statistics relate to the female athlete triad and the lack of awareness of RED-S in male athletes is even more marked. RED-S as a condition impacting males, as well as females, was described in the initial IOC consensus statement published in 2014. However there is evidence of the occurrence of RED-S in male athletes pre-dating this.
Identification
Identifying an athlete/dancer with RED-S is not always straight forward. In dance or sports where being light weight confers a performance or aesthetic advantage, how can a coach/teacher distinguish between athletes who have this type of physique “naturally” and those who have disordered eating and are at risk of RED-S? Equally, low energy availability could be a result either of intentional nutrition restriction to control body weight and composition, or an unintentional consequence of not matching an increase in energy expenditure (due to increased training load), with a corresponding increase in energy intake.
Performance effects
Performance is paramount to any athlete or dancer. Apart from physical ability, being driven and determined are important characteristics to achieve success. If weight loss is perceived as achieving a performance advantage, then this can become a competitive goal in its own right: in terms of the individual and amongst teammates. This underlies the interactive effect of psychological factors in the development and progression in the severity of RED-S.
There is both theoretical and practical evidence that short term low energy availability impairs athletic performance as the body is less able to undertake high quality sessions and benefit from the physiological adaptations to exercise. Within day energy deficits have been shown to have adverse effects in both male and female athletes in terms of impact on oestradiol/testosterone and cortisol concentrations. Failure to refuel with carbohydrate and protein promptly after a training session in male runners has been shown to have an adverse effect on bone turnover markers.
To underline the adverse performance effect of low energy availability, a recent study demonstrated that in female athletes, those with functional hypothalamic amenorrhea displayed decreased neuromuscular performance compared to their eumenorrhoeic counterparts. This adverse effect on performance is of particular concern where such skills are crucial in precisely those sports/dance where RED-S is most prevalent. Clearly this situation puts such athletes at increased injury risk, especially if associated with adverse bone mineral density (BMD) due to low energy availability.
Ironically the long term consequences of low energy availability produce adverse effects on body composition: increased fat/lean and reduction in BMD. In other words, the precise opposite effects of what an energy restricted athlete is trying to achieve. In terms of bone health, the lumbar spine is most sensitive to nutrition/endocrine factors (apart from rowers where mechanical loading can attenuate BMD loss at this site in RED-S). Suboptimal BMD is associated with an increased risk of bone injury and therefore impaired performance.
Medical Assessment
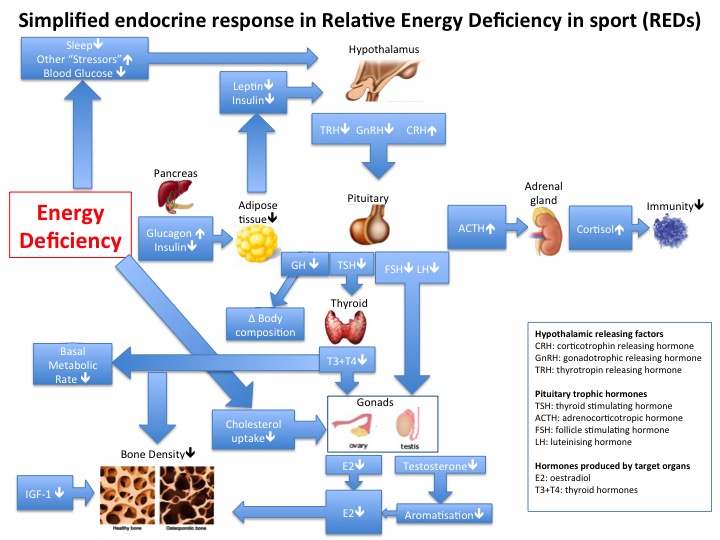
Low energy availability is the fundamental issue driving the multi-system dysfunction in the endocrine, metabolic, haematological, cardiovascular, gastrointestinal, immunological and psychological systems in RED-S. However, there are practical issues with directly quantifying energy availability as this is subject to the inaccuracies of reliably measuring energy intake and output. Endocrine and metabolic markers have been shown to more objective indicators of low energy availability, which in turn are correlated to performance outcomes such as bone stress injury in male and female athletes. In the case of female athletes there is an obvious clinical indicator of sufficient energy availability: menstrual cycles. As there is no such obvious clinical sign in male athletes is this why RED-S is less frequently recognised? In both female and male athletes there is some degree of clinical variation: there is no absolute threshold cut off with a set temporal component of low energy availability resulting in amenorrhoea or low testosterone in males. Therefore the IOC recoomends that individual clinical evaluation include discussion of nutrition attitudes and practices, combined with menstrual history for females and endocrine markers for male and female athletes will give a very clear indication if an athlete is at risk of/has RED-S.
Management
RED-S is a diagnosis of exclusion. Once medical conditions per se have been excluded, RED-S presents a multi-system dysfunction caused by a disrupted periodisation of nutrition/training/recovery. For an athlete the motivation to address these imbalances is to be in a position reach their full athletic potential. This attainment is compromised in RED-S.
Pharmacological interventions are not recommended as first line management in amenorrhoeic athletes. Oral contraception (OCP) masks amenorrhoea with withdrawal bleeds. OCP does not support bone health and indeed may exacerbate bone loss by suppressing further IGF-1. Although transdermal oestrogen, combined with cyclic progesterone does not down regulate IGF-1, nevertheless any hormonal intervention cannot be a long term solution, as bone loss will continue if energy availability is not addressed as a priority.
What next?
The IOC statement suggests further research should include studies with allocation of athletes to intervention groups, with assessment of effects over a substantial time period. Currently a study of competitive male road cyclists over a training/competition season is being undertaken to evaluate the effects of nutrition advice and off bike skeletal loading exercise. Crucially outcome measures will not only be based on bone health and endocrine markers, but measures of performance in terms of power production and race results.
To raise awareness and build support pathways as recommended in the IOC statement, this is an on going process which requires communication between athlete/dancers, coaches/teachers, parents and healthcare professionals both medical and non medical working with male and female athletes.
References
IOC consensus statement on relative energy deficiency in sport (RED-S): 2018 update BJSM 2018
Male Cyclists: bones, body composition, nutrition, performance BJSM 2018
Male Athletes: the Bare Bones of Cyclists
Addiction to Exercise – what distinguishes a healthy level of commitment from exercise addiction? BJSM 2017
Sports Endocrinology – what does it have to do with performance? BJSM 2017
Within‐day energy deficiency and reproductive function in female endurance athletes Scandinavian Journal of Science and medicine in Sports 2017
The Effect of Postexercise Carbohydrate and Protein Ingestion on Bone Metabolism Translational Journal of the American College of Sports Medicine 2017
Reduced Neuromuscular Performance in Amenorrheic Elite Endurance Athletes Medicine & Science in Sports & Exercise. 49(12):2478–2485, DEC 2017
Cumulative Endocrine Dysfunction in Relative Energy Deficiency in Sport (RED-S) BJSM 2018
Cyclists: Make No Bones About It BJSM 2018
Low Energy Availability is Difficult to Assess But Outcomes Have Large Impact on Bone Injury Rates in Elite Distance Athletes Sports Nutrition and Exercise Metabolism 2017
Part 2: Health, Hormones and Human Performance take centre stage BJSM 2018
Cyclists: How to Support Bone Health?
Healthy Hormones BASEM 2018