Keywords: tendinopathy, exercise therapy, resistance exercise dose
In this blog post we will summarise our recent study addressing what dose of resistance exercise is best for treating tendinopathy. This study was funded by the National Institute for Health Research (NIHR) as part of a large literature-based project on exercise therapy for the treatment of tendinopathy. The study was led by Robert Gordon University in collaboration with Queen Mary University of London, Barts Health NHS Trust, Sportscotland and NHS Grampian.
Why is this study important?
Tendinopathy is a common condition that involves degenerative changes in the tendons that link our muscles to bones. It is often seen in the Achilles (heel), elbow, rotator cuff (shoulder), patellar (knee) and hip tendons (Fu 2019). It happens in athletic and non-athletic people (Ackermann 2012) and results in persistent pain (Hopkins 2016, Scott 2020), swelling, reduced function and movement (Alizadehkhaiyat 2007). Exercise therapy is the leading conservative treatment for tendinopathy (Abat 2017, Alfredson 2005, O’Neill 2015).
We previously found that resistance exercise is most frequently prescribed (Cooper 2023), particularly eccentric exercise which loads the muscle during its lengthening phase. It is thought that by gradually encouraging tolerance to load, structural adaptations at the tendon and muscle tissue promotes recovery and restoration of function. As with any intervention, the effectiveness of resistance exercise is likely to be influenced by its dose, which can be described by the intensity, volume and frequency of exercise. While tendinopathy research has attempted to explore this dose-response relationship with resistance exercise, no clear recommendations have been made to date.
This study is important as we were able to investigate effects of resistance exercise dose components (including intensity, volume and frequency) across the most common tendinopathies (rotator cuff related shoulder pain (RCRSP), lateral elbow, patellar, gluteal and Achilles) using modern statistical approaches.
How did the study go about this?
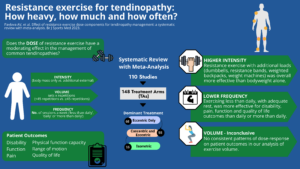
We performed a systematic review of studies that included resistance exercise interventions as the main treatment for any of the common tendinopathies. In addition to recording all the details of interventions we attempted to code each component of dose; intensity (body mass only or additional loads), volume (sets x repetitions) and frequency (number of sessions a week→ ‘less than daily’, ‘daily’ or ‘more than daily’). Meta-analyses and meta-regressions were used to explore relationships between dose components and patient outcomes including disability, pain, function and quality of life.
What did the study find?
We included 110 studies, with a total number of 3953 participants, that used resistance exercise therapy for treating tendinopathies. We found that higher intensity resistance exercises which involved using external loads (dumbbells, resistance bands, weighted backpacks, weight machines) were consistently more effective at improving patient outcomes compared with resistance exercise that relied on bodyweight only. It appears that some studies prescribing resistance exercise interventions were not sufficiently loaded to bring about the structural adaptations required for tendon repair (Gatz 2020, Cho 2017).
Interventions where resistance exercise was done less frequently, with rest days, had better outcomes for disability, pain, function and quality of life than those doing resistance exercises daily or more than once a day. This is consistent with strength training principles which call for rest days to encourage better adaptive processes in the mechanical properties of tendons before further loading occurs. The most common number of total repetitions was 45 (e.g., 3 sets of 15 repetitions) but we did not find any consistent patterns of dose-response on patient outcomes in our analysis of exercise volume.
What are the key take-home points?
Clinicians prescribing resistance exercise should consider including higher intensities, that involve adding external weight, and should ensure adequate rest between sessions to facilitate recovery. Although some patients may need a longer period to build up their intensity it is important to keep reviewing whether the load intensity is adequate to trigger improvements.
References:
- Fu FH, Wang JC, Rothrauff BB. Best practice tendinopathy. BMJ. 2019.
- Ackermann PW , Renström P . Tendinopathy in sport. Sports Health 2012;4:193–201. doi:10.1177/1941738112440957
- Hopkins C , Fu S-C , Chua E , et al . Critical review on the socio-economic impact of tendinopathy. Asia Pac J Sports Med Arthrosc Rehabil Technol 2016;4:9–20. doi:10.1016/j.asmart.2016.01.002
- Scott A , Squier K , Alfredson H , et al . Icon 2019: international scientific tendinopathy symposium consensus: clinical terminology. Br J Sports Med 2020;54:260–2. doi:10.1136/bjsports-2019-100885
- Alizadehkhaiyat O , Fisher AC , Kemp GJ , et al . Pain, functional disability, and psychologic status in tennis elbow. Clin J Pain 2007;23:482–9. doi:10.1097/AJP.0b013e31805f70fa
- Abat F , Alfredson H , Cucchiarini M , et al . Current trends in tendinopathy: consensus of the ESSKA basic science Committee. Part I: biology, biomechanics, anatomy and an exercise-based approach. J Exp Orthop 2017;4:18. doi:10.1186/s40634-017-0092-6
- Alfredson H . The chronic painful Achilles and Patellar tendon: research on basic biology and treatment. Scand J Med Sci Sports 2005;15:252–9. doi:10.1111/j.1600-0838.2005.00466.x
- O’Neill S , Watson PJ , Barry S . Why are eccentric exercises effective for Achilles tendinopathy? Int J Sports Phys Ther 2015;10:552–62.
- Cooper K, Alexander L, Brandie D, Brown VT, Greig L, Harrison I, MacLean C, Mitchell L, Morrissey D, Moss RA, Parkinson E, Pavlova AV, Shim J, Swinton PA (2023). Exercise therapy for tendinopathy: a mixed methods evidence synthesis exploring feasibility, acceptability and effectiveness. Health Technology Assessment (in press) https://doi.org/10.3310/TAHK7102
- Gatz M, Betsch M, Dirrichs T, et al. Eccentric and Isometric Exercises in Achilles Tendinopathy Evaluated by the VISA-A Score and Shear Wave Elastography. Sports Health 2020;12:373-81.
- Cho S, Shin Y. Effect of rehabilitation and prolotherapy on pain and functional performance in patients with chronic patellar tendinopathy. Gazzetta Medica Italiana Archivio per le Scienze Mediche 2017;176:330-337.
Original Article: Pavlova AV, Shim JSC, Moss R, et al. Effect of resistance exercise dose components for tendinopathy management: a systematic review with meta-analysis. British Journal of Sports Medicine, Published Online First: 11 May 2023. doi: 10.1136/bjsports-2022-105754
Correspondence: Dr Anastasia Pavlova, Research Fellow, School of Health Sciences, Robert Gordon University, Aberdeen (UK); a.pavlova1@rgu.ac.uk
Related Links:
RGU Project page: https://rgu-repository.worktribe.com/project/230179/exercise-therapy-for-the-treatment-of-tendinopathies
NIHR Project page: https://dev.fundingawards.nihr.ac.uk/award/NIHR129388
NIHR Health Technology Assessment report: Cooper K, Alexander L, Brandie D, Brown VT, Greig L, Harrison I, MacLean C, Mitchell L, Morrissey D, Moss RA, Parkinson E, Pavlova AV, Shim J, Swinton PA (2023). Exercise therapy for tendinopathy: a mixed methods evidence synthesis exploring feasibility, acceptability and effectiveness. Health Technology Assessment (in press) https://doi.org/10.3310/TAHK7102
BMJ Open: Effect Size paper https://bmjopensem.bmj.com/content/9/1/e001389