Part of the BJSM’s #KnowledgeTranslation blog series
In the following blog we summarise the main finding of our two recent papers examining the effect of β2-agonists on physical performance1,2. We found that β2-agonists may improve anaerobic but not aerobic performance in healthy athletes.
Asthma is common in top athletes3 and β2-agonists are often prophylaxis for exercise induced bronchial constriction (EIB), and as a reliever for symptoms4. Asthmatic athletes have consistently outperformed their non-asthmatic peers5, and this has led to speculation regarding a possible performance enhancing effect of β2-agonists. Thus, the World Anti-Doping Agency (WADA) have banned the use of all β2-agonists (apart from the use of some β2-agonists inhaled in low doses6).
Numerous studies have investigated the effect of different types, doses, administration routes and treatment durations of β2-agonists on various types of maximal physical performance and the results have been conflicting. Therefore, we wanted to systematically review and meta-analyse these studies to investigate new and more complete patterns in the effect of β2-agonists on physical performance in healthy athletes.
Meta-analysis of randomised controlled trials
We screened four scientific databases for randomised controlled trials assessing the effect of β2-agonists on maximal physical performance and assessed bias according to the recommendations from the Cochrane Collaboration. We categorised β2-agonists according to type, dose, administration routes and treatment durations. The primary outcomes were anaerobic performance and aerobic performance. Anaerobic performance was subcategorised into strength, power and sprint performance, and aerobic performance was subcategorised into maximal oxygen uptake (VO2max) and physical aerobic performance. We performed meta-analyses with meta regression.
Different effects on anaerobic and aerobic performance
We found 81 studies comprising 1152 participants, finding no difference in effect between studies with high and low risk of bias.
Overall β2-agonists improved anaerobic performance by 5%. In stratified analyses both sprint performance and maximal muscular strength were improved by β2-agonists. When we assessed the effect of doses approved and prohibited by WADA separately, prohibited doses improved anaerobic performance or strength and sprint performance analysed separately. Approved doses did not improve anaerobic performance or sprint and strength performance (Infographic 1). However, there was a tendency towards improved anaerobic performance also by WADA approved doses (p=0.051).
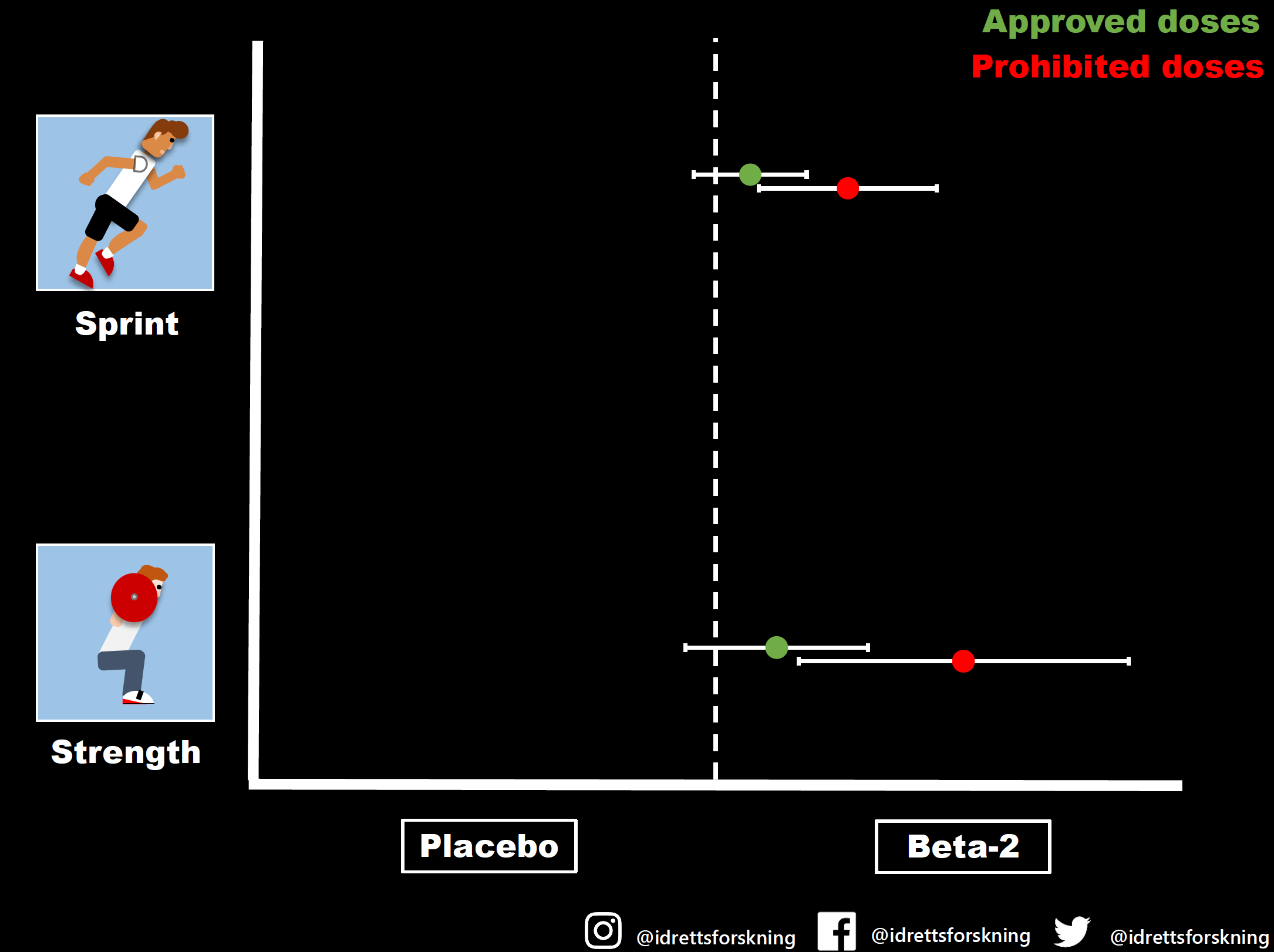
Infographic 1: The effect of β2-agonists on strength and sprint performance stratified by dose. (If the whiskers cross the dotted line the effect is zero)
Aerobic performance was not affected by the use of β2-agonists in the overall analysis or any analysis examining the effect of dose, type, administration routes or treatment durations on aerobic performance or when aerobic performance was divided into physical performance, time trial performance, time to exhaustion or VO2max (Infographic 2).
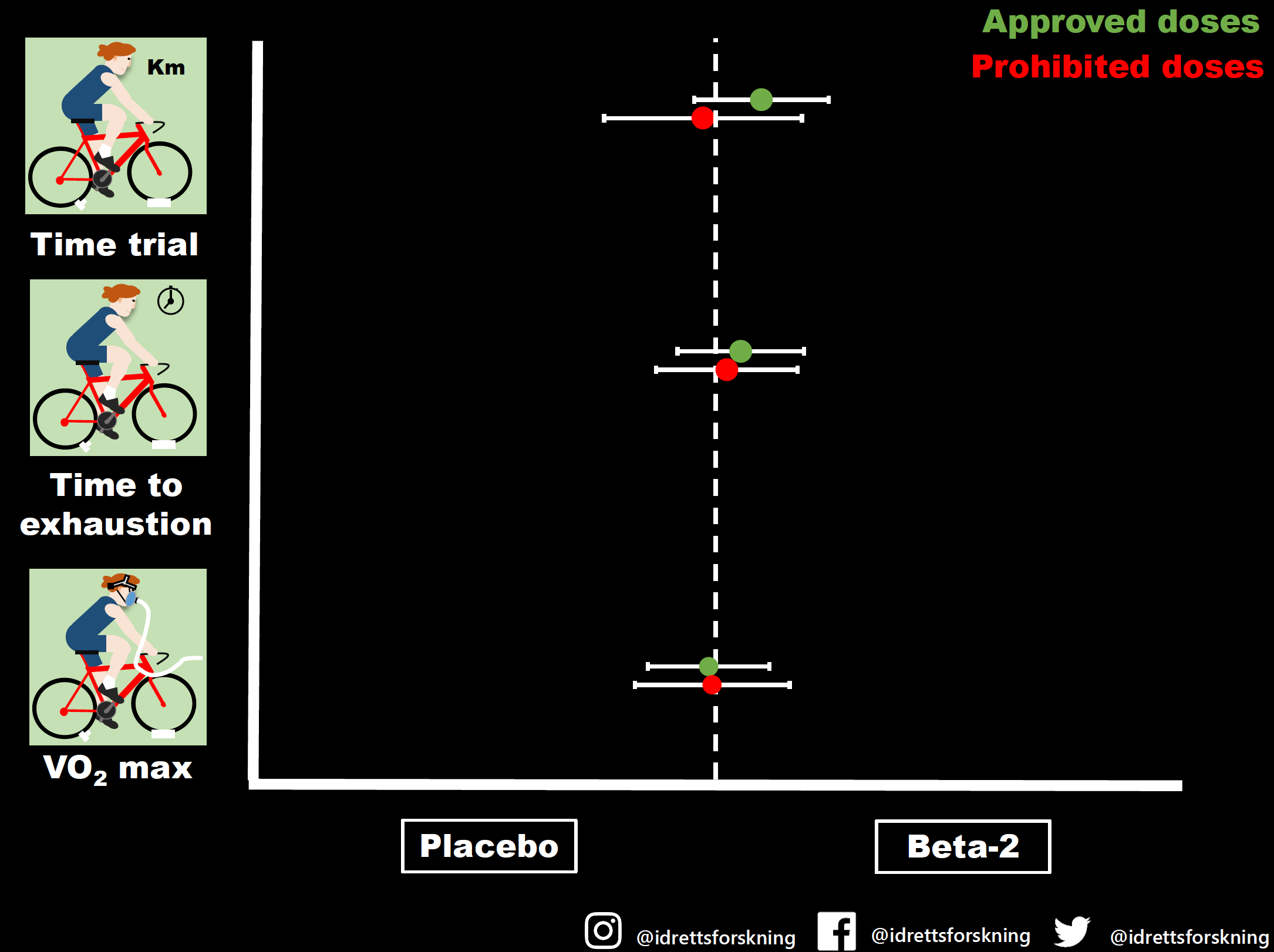
Infographic 2: The effect of β2-agonists on time to exhaustion, time trial performance and VO2max stratified by dose. (If the whiskers cross the dotted line the effect is zero)
The effect is dose dependent, what are the other take-home points?
- Anaerobic performance, such as strength and sprint, can be improved in healthy athletes using β2-agonists, with the effect is dependent on the dose.
- It is unclear whether WADA approved doses can improve anaerobic performance.
- Endurance performance was not affected by β2-agonists regardless of type, dose, administration routes and treatment durations, or how endurance was tested.
- Our results indicate that the differentiation between approved and illegal doses is meaningful as their effect differs, but as the effect of approved doses is unclear, more regulations such as documentation of asthma with objective tests before use of any β2-agonists should be considered.
- As we did not find any effect of β2-agonists on endurance performance, the sport authorities may perhaps shift their focus regarding abuse of β2-agonists from endurance sports to strength and speed events (especially if they must prioritise their resources.)
In light of the present studies future research should seek to determine the effect of approved doses of β2-agonists on strength, sprint and power performance in healthy athletes and if sprint ability within an endurance test (to simulate explosive accelerations within a bicycle race or a cross country ski race) is improved by β2-agonists.
Authors and Affiliations:
Amund Riiser1, Trine Stensrud2, Julie Stang2, Lars Bo Andersen1
Infographics: Matthew Shaw / Idrettsforskning1
1 Faculty of Teacher Education, Art and Sport, Western Norway University of Applied Sciences, Sogndal, Vestland, Norway
2 Department of Sports Medicine, Norwegian School of Sport Sciences, Oslo, Norway
Correspondence to Dr Amund Riiser, Faculty of Teacher Education, Art and Sport, Western Norway University of Applied Sciences, Sogndal, Vestland, Norway; amund.riiser@hvl.no
The authors declare no conflict of interest
References:
- Riiser A, Stensrud T, Stang J, et al Can β2-agonists have an ergogenic effect on strength, sprint or power performance? Systematic review and meta-analysis of RCTs. British Journal of Sports Medicine Published Online First: 03 August 2020. doi: 10.1136/bjsports-2019-100708
- Riiser A, Stensrud T, Stang J, et al Aerobic performance among healthy (non-asthmatic) adults using beta2-agonists: a systematic review and meta-analysis of randomised controlled trials. British Journal of Sports Medicine Published Online First: 14 August 2020. doi: 10.1136/bjsports-2019-100984
- McKenzie DC, Fitch KD. The asthmatic athlete: inhaled beta-2 agonists, sport performance, and doping. Clin J Sport Med 2011;21:46–50.doi:10.1097/IAE.0b013e318203c0efpmid:http://www.ncbi.nlm.nih.gov/pubmed/21200170
- Global Initiative for Asthma. Global strategy for asthma management and prevention, 2020. Available: www.ginasthma.org [Accessed 27 aug 2020].
- Fitch KD. An overview of asthma and airway hyper-responsiveness in Olympic athletes. Br J Sports Med 2012;46:413–6.doi:10.1136/bjsports-2011-090814pmid:http://www.ncbi.nlm.nih.gov/pubmed/22228581
- World Anti-Doping Agency. Prohibited list, 2020. Available: https://www.wada-ama.org/sites/default/files/wada_2020_english_prohibited_list_0.pdf [Accessed 17 Feb 2020].