Keywords: physical activity, low- and middle-income countries, behaviour change, digital health, policy, systematic review
The short answer is yes! The improvements are usually small, but they are real and meaningful when applied across large populations. In this blog, we discuss our recent study published in the British Journal of Sports Medicine (1).
Why is this study important?
Physical inactivity is a major cause of non-communicable diseases such as heart disease, diabetes, and some cancers worldwide (2). These conditions are rising quickly in low- and middle-income countries (LMICs), where more than 80% of the world’s population lives (3). Yet most physical activity guidelines and programme designs come from high-income countries. That makes it harder for clinicians and policymakers in LMICs to know what works best in their own settings.
It is also important to recognise that “being inactive” looks different across contexts. Many adults in LMICs already have physically demanding work. At the same time, safe and structured options for leisure-time activity may be limited by city design, traffic, safety concerns, cultural norms, and lack of facilities. So, the key question is straightforward: do physical activity programmes actually work in LMICs, and if so, what makes them effective?
How did the study go about this?
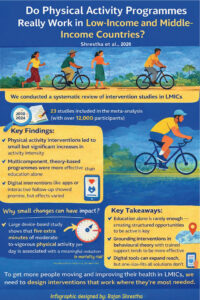
We conducted a systematic review and meta-analysis of randomised controlled trials and quasi-experimental studies published between 2010 and 2024. After searching four major databases, we identified 43 eligible studies conducted in LMICs. Of these, 23 provided sufficient data for meta-analysis, representing more than 12,000 participants across community, primary care and workplace settings.
We looked at changes in:
- activity intensity measured as metabolic equivalent (MET) minutes,
- time spent in moderate-to-vigorous physical activity (minutes/week)
- time spent in sedentary behaviour (minutes/day)
Because the studies varied widely in design, populations and delivery approaches, we used statistical methods that account for this variation and assessed how strong and reliable the evidence was.
A major gap stood out: none of the included studies was from low-income countries.
What did the study find?
Overall, physical activity programmes in LMICs led to small but statistically significant increases in activity intensity. However, they had little impact on total activity time or sedentary behaviour. In simple terms, people tended to move more vigorously, but not necessarily for longer and sitting time did not consistently change.
Some approaches appeared more effective than others:
- Education plus structured or supervised activity tended to work better than education alone.
- Programmes using behaviour-change theory looked more promising.
- Digital components (for example apps, messaging, or interactive follow-up) helped in some settings, especially as reminders and support
There were also limitations. Many studies relied on self-reported activity, and there was considerable variation between studies, which means overall confidence in the findings remains limited.
What are the key take-home points?
Small effect sizes can still matter. The biggest relative health gains often happen among people who are least active. Evidence from large device-based cohort studies suggests that even about five extra minutes per day of moderate-intensity activity is associated with meaningful reductions in mortality risk. Going from no activity to some activity can therefore bring substantial benefit, and population-wide changes add up.
Several lessons stand out for LMICs:
- Education alone is rarely sufficient; programmes should include structured opportunities to practise physical activity.
- Behaviour-change principles and trained support are essential.
- Digital tools can extend reach and reinforce behaviour change but are not a stand-alone solution.
- Measurement enhances credibility; if accelerometers are not feasible, step counters or phone-based tracking can still support evaluation and accountability.
- Interventions must be adapted to local cultural, social, and environmental realities rather than copied directly from high-income settings.
Future studies should use better measurements, longer follow-up, and include low-income countries. The priority is no longer only asking whether programmes work but designing programmes that work in the places with the greatest need.
Contributors
Rajan Shrestha, Susan Paudel, Tara Ballav Adhikari, Bijay Khatri, Santoshi Adhikari, Dinesh Neupane, Abhinav Vaidya, Per Kallestrup, Anupa Rijal
References
- Shrestha R, Paudel S, Adhikari TB, et al. Effectiveness of physical activity promotion interventions in low-income and middle-income countries: a systematic review and meta-analysis. British Journal of Sports Medicine 2026;60:286-299.
- Lee IM, Shiroma EJ, Lobelo F, et al. Effect of physical inactivity on major non-communicable diseases worldwide: an analysis of burden of disease and life expectancy. Lancet 2012;380(9838):219-29.
- Mahler DG, Holla A, Serajuddin U. 2024. Available from: https://blogs.worldbank.org/en/opendata/time-stop-referring-developing-world#:~:text=In%20the%20World%20Bank%2C%20this,84%25%20of%20the%20world’s%20population.