How muscle loss affects ageing – and how physical activity promotes power, mobility, and independence
Key words: Sarcopenia, muscle strength, awareness
Introduction
There are several changes within different body systems that are associated with ageing. Some present obviously and others can be more quiescent. Sarcopenia is an indolent loss of muscle mass and strength over time which can lead to impairments in mobility and quality of life if not tackled. This initial blog of a 3 part series will aim to improve understanding of what sarcopenia is, the associated risks, why it matters and methods to manage this as it can affect those of varying ages (Figure 1).
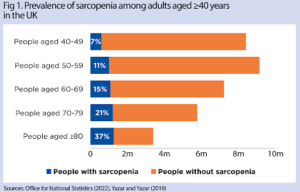
Fig. 1- Prevalence of those in the UK with sarcopenia [1]
Sarcopenia
Sarcopenia is a slow, progressive skeletal muscle disorder characterized by loss of muscle mass and strength that typically begins in midlife, with muscle mass declining on average by around 1–2% per year from about age 50 [2]. It is an important mechanism linking ageing with frailty – a state of system-wide physiological vulnerability – and with increased falls and fracture risk, yet it often remains under-recognised in the clinical assessment of older adults [3].
The process can begin as early as midlife with risk factors including a sedentary lifestyle, smoking and alcohol use, poor dietary intake, multimorbidity, polypharmacy, recent extended hospital stays and social isolation [4].
Patients will also commonly present with generalised slowing down, loss of confidence in their physical capabilities or avoidance of specific activities after an acute incident such as a fall – this often results in a very unpredictable recovery process [4].
There are several risks associated with this pathological process. The reduction in muscle mass can add to the risk of falls, fractures and significant reduction in the ability to carry out activities of daily living thus reducing quality of life and causing psychological distress to both patients and carers [5]. Sarcopenia can lead to a greater overall mortality rate for patients [6]. Additionally, in cases of patients with an elevated BMI at baseline, the term “sarcopenic obesity” is used and this leads to an exacerbation of the health risks outlined above [7].
As stated, the earlier sarcopenia can be identified, the better outcomes can be [8]. However, significant under-diagnosis is a challenge in sarcopenia management. There are a variety of questionnaires such as SARC-F used, coupled with some objective muscle testing such as sit to stand test to allow early assessment as well as looking at walking speed as a functional measure [9]. While there are no blood tests that can confirm or refute a diagnosis, bloods can be used to establish risk or identify contributing factors such as underlying disease or vitamin deficiency. More sophisticated techniques such as dual‑energy X‑ray absorptiometry (DEXA/DXA) are required to make more accurate measurements of body composition, including lean mass and fat mass in addition to bone mineral density [4].
Why it matters
With an improvement in awareness and understanding of sarcopenia, comes far more timely and tailored interventions. The key intervention is a well-structured, supervised progressive strength training programme [10]. Sarcopenia management can be achieved in any age group and any functional capacity if carried out in a tailored way. The Chief Medical Officer guidance suggests aiming towards 150 minutes of moderate exercise per week, which should include twice weekly strength sessions alongside other forms of exercise [11]. More specifically, resistance training targets muscle fibres to enhance protein synthesis which promotes hypertrophy and improved function [12]. Patients using GLP-1 agonists indicated for metabolic/obesity related conditions, however, lean mass loss is a concern during weight loss; therefore resistance training and adequate protein are essential adjuncts [7].
The benefits of resistance training go beyond physical function and can help to improve prevention and/or management of chronic diseases such as diabetes, cardiovascular disease, osteoporosis and tempering overall frailty [13].
It is important the focus remains on muscle mass and function rather than looking at the number on the scales, however these aspects will be tackled more extensively in part 2. Additionally, the rarity of sarcopenia occurring in isolation argues strongly for a holistic approach that encompasses a full and comprehensive geriatric assessment from a frailty specialist [14].
Image 1: demonstration of muscle loss over time in Sarcopenia
Conclusions
- Sarcopenia is an important diagnosis that is often missed and overlooked which, if recognised, can play a pivotal role in reduced overall frailty and mortality levels in the elderly population
- It is not an inevitable but modifiable condition that with supervised resistance training can lead to improvements in muscle function and personal independence but also improvements in management and control of complex multimorbidity.
- Early intervention with education to patients and family members around the modifiable risk factors that can accelerate the process such as nutrition, alcohol and smoking can significantly enhance disease prevention.

Authors
Dr Callum Innes – ST3 Sport and Exercise Medicine and GP
Dr Tom Leggett – Para Football, Lead Performance Doctor, The FA; GP and SEM Physician
Dr Andrew Shafik – Club Doctor Chelsea FC, GP and SEM Physician
Dr Malin Farnsworth – Frailty Consultant, Epsom and St Helier University Hospitals NHS Trust
References
- Yazar, T. and H. Olgun Yazar, Prevalance of sarcopenia according to decade. Clin Nutr ESPEN, 2019. 29: p. 137–141.
- Wilkinson, D.J., M. Piasecki, and P.J. Atherton, The age-related loss of skeletal muscle mass and function: Measurement and physiology of muscle fibre atrophy and muscle fibre loss in humans. Ageing Res Rev, 2018. 47: p. 123–132.
- Sayer, A.A. and A. Cruz-Jentoft, Sarcopenia definition, diagnosis and treatment: consensus is growing. Age Ageing, 2022. 51(10).
- Sayer, A.A., et al., Sarcopenia. Nature Reviews Disease Primers, 2024. 10(1): p. 68.
- Beaudart, C., et al., Health Outcomes of Sarcopenia: A Systematic Review and Meta-Analysis. PLoS One, 2017. 12(1): p. e0169548.
- Guralnik, J.M., et al., A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. Journal of gerontology, 1994. 49(2): p. M85–M94.
- Sargeant, J.A., et al., A Review of the Effects of Glucagon-Like Peptide-1 Receptor Agonists and Sodium-Glucose Cotransporter 2 Inhibitors on Lean Body Mass in Humans. Endocrinol Metab, 2019. 34(3): p. 247–262.
- Xie, W.Q., et al., Possible sarcopenia: early screening and intervention-narrative review. Ann Palliat Med, 2020. 9(6): p. 4283–4293.
- Bohannon, R.W., et al., Grip and knee extension muscle strength reflect a common construct among adults. Muscle Nerve, 2012. 46(4): p. 555–8.
- Hurst, C., et al., Resistance exercise as a treatment for sarcopenia: prescription and delivery. Age Ageing, 2022. 51(2).
- GOV, U., Physical activity guidelines: UK Chief Medical Officers’ report. 2019.
- Shen, Y., et al., Exercise for sarcopenia in older people: A systematic review and network meta-analysis. J Cachexia Sarcopenia Muscle, 2023. 14(3): p. 1199–1211.
- Gao, Q., et al., Associated Factors of Sarcopenia in Community-Dwelling Older Adults: A Systematic Review and Meta-Analysis. Nutrients, 2021. 13(12).
- Parker, S.G., et al., What is Comprehensive Geriatric Assessment (CGA)? An umbrella review. Age Ageing, 2018. 47(1): p. 149–155.