Osteoarthritis (OA) is the most prevalent joint disease with a fifth of people aged over 45 years developing knee OA in their lifetime [1].
Many patients are often told to wait until they are candidates for total knee arthroplasty (TKA) without receiving symptomatic relief. This is because arthroplasty is relatively contraindicated without full thickness chondral loss or “bone on bone” contact. Younger, more active patients often fall into this treatment gap. TKA in this group also carries a higher risk of revision surgery and dissatisfaction due to the loss of native knee kinematics.
When arthroplasty is indicated, the vast majority of patients (85%) undergo TKA replacing the entire joint [2]. However, based on a meta-analysis by Stoddart et al., only a quarter of patients with knee OA have tricompartmental disease [3]. There is therefore a large number of patients with unicompartmental disease being overtreated with TKA. Overuse of TKA exposes patients to an increased risk of serious complications such as thromboembolism, myocardial infarction, and stroke as well as increased costs [4].
There is clearly a requirement to raise awareness amongst patients and healthcare professionals from all specialties of the prevalence of unicompartmental knee OA and the current evidence-based knee preservation therapies available for this large cohort of patients. The infographic (figure 1) summarises and consolidates guidelines from a recent consensus statement on osteotomies around the knee [5], an algorithm paper for medial knee pain [6] as well as NICE guidelines on the management of OA [7].
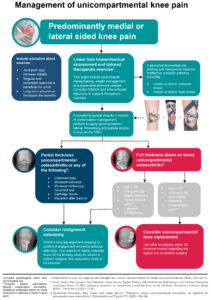
Figure 1 Infographic summary
Exercise and Education
Exercise and education, prescribed as part of a physiotherapy program, are the recommended first-line treatments for people diagnosed with knee OA. Physiotherapy however remains extremely underutilized for the management of arthritic pain and delayed initiation has recently been associated with a higher risk of opioid use in patients with knee OA [8].
- Cartilage strain and activity
Articular cartilage (AC) is composed of chondrocytes bound together by an extracellular matrix (ECM). Its function is to support and distribute load-bearing forces in joints and to reduce friction by providing a smooth lubricated surface. AC has poor healing potential however and is prone to both acute injury and degenerative disease. This may be exacerbated by excessive load or maldistribution of load within the joint [9].
Magnetic resonance imaging in combination with high-speed dual-fluoroscopy, has shown that during normal activities, diurnal strains upon the AC range from 010 %, post-activity strains range from 5-15 %, and dynamic strains during activity, such as a short bout of running, range from 15-35 % with greater strains seen on the medial side of the joint [10]. Higher strain magnitudes of 50–70 % are detrimental and can cause cartilage injury, with levels above 70% inducing cell death via necrosis and apoptosis.
- Changes in Chondrocyte function in response to exercise
Exercise induced physiologic dynamic strain of AC (at 15-35%) decreases the expression of catabolic and pro-inflammatory genes and enhances synthesis of ECM components such as proteoglycans, collagens, and cartilage oligomeric matrix protein [11]. Higher strain magnitudes lead to direct cellular damage as well as pathologic loss of ECM constituents through the enhancement of catabolic enzymes [12] (figure 2). Similarly, the absence of normal joint loading also leads to the inhibition of ECM synthesis resulting in thinner and softer AC, which in turn is more susceptible to trauma and degenerative changes [13]. These findings may account for the association of osteoarthritis (OA) with a more sedentary lifestyle and the lower incidence of OA in recreational runners [14].
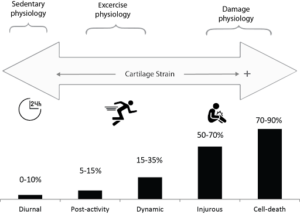
Figure 2 Diurnal, post-activity, dynamic during activity, and damage inducing cartilage strains [9]
Coronal plane alignment and its association with medial knee pain
The Knee Adduction Moment (KAM) is an indirect measure of medial knee load during walking and is calculated as the product of the ground reaction force (GRF) in the frontal plane and the perpendicular distance of the GRF to the knee joint centre of rotation, called the frontal plane lever arm[15] (Figure 3).
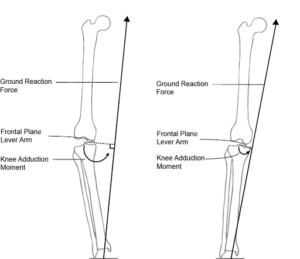
Figure 3 The knee adduction moment during walking. This is higher in the presence of varus (left) vs. valgus (right) alignment [9].
An increased KAM has been related to increased medial knee pain and radiographic OA severity as well as faster OA progression [16]. To prevent the progression of AC loss and medial knee symptoms, various interventions have focussed on reducing either the GRF and or the lever arm that produces the KAM. Conservative measures include weight loss and strengthening of the muscles around the knee. Villagizing knee braces have been shown to effectively reduce the KAM and improve symptoms of medial knee arthritis[17]. Surgically, valgus producing realignment osteotomy is a robust method of manipulating the lever arm and can be a powerful tool in reducing the KAM in patients who have failed conservative methods [18].
Realignment osteotomy
In the late twentieth century, the popularity of knee osteotomy faded with the evolution of arthroplasty. However, we have since witnessed a significant resurgence of osteotomy practice over the course of the last 20 years following advances in the planning of corrections, the utilization of angular stable fixation devices and accelerated rehabilitation regimens. Compared to arthroplasty, osteotomy better retains native knee kinematics and is thus better suited for those interested in returning to impact sport [19]. This along with other indications for realignment osteotomy in the context of knee pathology were defined in a recent UK consensus paper [5]. Realignment osteotomy can be performed above or below the joint with opening or closing wedges most commonly performed.
Unicompartmental knee replacement
Unicompartmental knee arthroplasty (UKA) preserves a significant proportion of the unaffected chondral surfaces in the knee, as well as the proprioceptive components including the cruciate ligaments. This likely contributes to better functional outcomes, shorter length of stay, quicker recovery, less blood loss and lower mortality compared to TKA [20]. The National Institute for Health and Care Excellence (NICE) therefore recommends that UKA is considered in patients with uni-compartmental knee OA as an alternative to TKA [21].
Although UKA and realignment osteotomy are both knee preserving surgeries in the treatment of unicompartmental disease, they have differing ideal indications and optimal outcomes are only achieved with careful patient selection . Younger patients with partial thickness disease and bony deformity are generally better treated with realignment osteotomy, whereas older patients with more advanced intra-articular disease and correctable deformity are more suited to UKA [6].
Conclusion
The refinement of total knee arthroplasty has resulted in good clinical results for most elderly patients with advanced joint disease. Younger patients with higher activity levels and expectations are better suited to therapies that maintain the biological envelope of the knee particularly in isolated unicompartmental knee disease where a wider spectrum of effective therapies is available. The infographic presented (figure 1) serves as a useful summary tool for healthcare professionals and patients with the aim of guiding clinical practice to improve the quality of life for this large group of patients.
Authors and affiliations: Osama Aweid, Firas Raheman, Simon Lack, Nat Padhiar, Sam Yasen, Matthieu Olliviere
Mr Osama Aweid
MBBS BSc (hons) MSc (SEM) FRCS (Orth) MFSEM (UK)
Consultant Knee and Sports Medicine Surgeon
1)Fortius Clinic, London, UK
2)The London Independent Hospital, Stepney Green, London, UK.
3) Broomfield Hospital, Mid and South Essex NHS Trust, Chelmsford, UK
Mr Firas Raheman
MD(res) MSc(Dist) MRCS MAcadMEd
Specialty Registrar in Trauma and Orthopaedics
1)Broomfield Hospital, Mid and South Essex NHS Trust, Chelmsford, UK
Professor Nat Padhiar
MSc PhD FCPodS
Consultant Podiatric Surgeon & Honorary Reader
1)Centre for Sports and Exercise Medicine, Barts and the London School of Medicine and Dentistry, Mile End Hospital, Queen Mary University of London, London, E1 4DG, England.
Dr Simon Lack
PhD, MSc, BSc
Advanced Physiotherapy Practitioner
1)Centre for Sports and Exercise Medicine, Barts and the London School of Medicine and Dentistry, Mile End Hospital, Queen Mary University of London, London, E1 4DG, England.
2)Pure Sports Medicine, Point West Building, London, United Kingdom.
Mr Sam Yasen
MBBS, BSc, MSc (Eng), MRCS, FRCS (Tr & Orth), PCGE, FHEA, MFSEM
Trauma and Orthopaedic Consultant
1)Basingstoke & North Hampshire Hospital, Basingstoke, UK
Dr Matthieu Olliviere
MD, PhD, MSc
Trauma and Orthopaedic Consultant
1)Aix-Marseille University, CNRS, Marseille, France.
2) APHM, Institute for Locomotion, Sainte-Marguerite Hospital, Department of Radiology, Marseille, France.
References
- UK, A.R. and I.C. London, The musculoskeletal calculator. 2014.
- Achakri, H., et al., The National Joint Registry 20th Annual Report 2023 [Internet]. 2022.
- Stoddart, J., et al., The compartmental distribution of knee osteoarthritis–a systematic review and meta-analysis. Osteoarthritis and cartilage, 2021. 29(4): p. 445-455.
- Liddle, A.D., et al., Adverse outcomes after total and unicompartmental knee replacement in 101 330 matched patients: a study of data from the National Joint Registry for England and Wales. The Lancet, 2014. 384(9952): p. 1437-1445.
- Snow, M., et al., A 2021 consensus statement on osteotomies around the knee by the UK Knee Osteotomy consensus Group (KOG). The Knee, 2021. 33: p. 73-83.
- Vipulendran, K., S. Yasen, and J. Murray, Osteotomy versus unicompartmental arthroplasty: an algorithm for anteromedial knee osteoarthritis. Orthopaedics and Trauma, 2023. 37(3): p. 184-194.
- guideline NG226, N., Osteoarthritis in over 16s: diagnosis and management. Methods, 2022.
- Kumar, D., et al., Delayed timing of physical therapy initiation increases the risk of future opioid use in individuals with knee osteoarthritis: a real-world cohort study. British Journal of Sports Medicine, 2023. 57(15): p. 958-964.
- Aweid, O., L. Batty, and A.M.J. Getgood, The Role of Alignment Correction With and Without Chondral Repair, in Early Osteoarthritis: State-of-the-Art Approaches to Diagnosis, Treatment and Controversies, C. Lattermann, et al., Editors. 2022, Springer International Publishing: Cham. p. 247-258.
- Sanchez-Adams, J., et al., The mechanobiology of articular cartilage: bearing the burden of osteoarthritis. Current rheumatology reports, 2014. 16(10): p. 451.
- O’Conor, C.J., et al., TRPV4-mediated mechanotransduction regulates the metabolic response of chondrocytes to dynamic loading. Proceedings of the National Academy of Sciences, 2014. 111(4): p. 1316-1321.
- Musumeci, G., The effect of mechanical loading on articular cartilage. 2016, Multidisciplinary Digital Publishing Institute.
- Ruberti, J.W. and N.J. Hallab, Strain-controlled enzymatic cleavage of collagen in loaded matrix. Biochemical and biophysical research communications, 2005. 336(2): p. 483-489.
- Alentorn-Geli, E., et al., The association of recreational and competitive running with hip and knee osteoarthritis: a systematic review and meta-analysis. journal of orthopaedic & sports physical therapy, 2017. 47(6): p. 373-390.
- Zhao, D., et al., Correlation between the knee adduction torque and medial contact force for a variety of gait patterns. Journal of orthopaedic research, 2007. 25(6): p. 789-797.
- Foroughi, N., R. Smith, and B. Vanwanseele, The association of external knee adduction moment with biomechanical variables in osteoarthritis: a systematic review. The Knee, 2009. 16(5): p. 303-309.
- Yan, Y., et al., Biomechanical effect of valgus knee braces on the treatment of medial gonarthrosis: a systematic review. Applied Bionics and Biomechanics, 2022. 2022(1): p. 4194472.
- Birmingham, T., et al., Changes in biomechanical risk factors for knee osteoarthritis and their association with 5-year clinically important improvement after limb realignment surgery. Osteoarthritis and cartilage, 2017. 25(12): p. 1999-2006.
- Jacquet, C., et al., Opening wedge high tibial osteotomy allows better outcomes than unicompartmental knee arthroplasty in patients expecting to return to impact sports. Knee Surgery, Sports Traumatology, Arthroscopy, 2020. 28(12): p. 3849-3857.
- Geller, J.A., R.S. Yoon, and W. Macaulay, Unicompartmental knee arthroplasty–A controversial history and a rationale for contemporary resurgence. The journal of knee surgery, 2008. 21(01): p. 7-14.
- guideline NG157, N., Joint replacement (primary): hip, knee and shoulder. Methods, 2020.