Authors: Paolo Perna and Marco Beato
Hamstring injuries continue to be the most common muscle injury in professional football. Despite the practitioners’ efforts, the high re-injury rate remains an issue (1). This makes the Return-to-Play (RTP) decisions even more challenging and increases the pressure on the medical and performance departments to clear players to return to training and play (faster but with limited risk). Frequently, RTP protocols consider hamstring injuries as one, and the severity and individual characteristics of the injuries are not taken into account. This blog aims to start thinking about RTP criteria based on the specific characteristics of a hamstring injury.
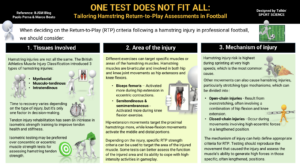
Specifically, we are going to look at three characteristics of hamstring injuries:
- Tissues involved
- Area of the injury
- Mechanism of injury
Tissues involved
Are all hamstring injuries equal? (2) The question started to be answered by the publication of the British Athletics Muscle Injury Classification (BAMIC) (3) with the definition of three types of injuries based on the tissue involved: myofascial, musculo-tendinous and intratendinous. Time is the first criterion to consider, and it could change depending on the type of injury (4). Although interesting to know, time is a small piece of the puzzle and is not enough to improve our decision-making. Tendon injury rehabilitation has seen an increase in the use of isometric strength to target tendon health and stiffness. Therefore, we could prefer isometric testing over concentric or eccentric muscle strength tests when we look at ways to test hamstring tendon strength functionally. This is only the first aspect of this individualised approach because the same tissue can be injured in different areas of the muscles.
Area of the injury
Several studies have highlighted how different exercises can target a specific muscle or area of the muscle. Hamstring muscles are bi-articular, so they act on the movement of the hip and knee joints as hip extensors and knee flexors. Bourne and colleagues showed that during eccentric contractions, the lateral hamstring (biceps femoris) is more selectively activated by the hip-extension movement, while the medial hamstrings (semitendinosus and semimembranosus) by the knee-flexion movement (5). Furthermore, the hip-extension movements can target more the proximal area of the hamstrings compared to the knee-flexion movements which showed a greater activation of the middle and distal portions of the muscles (6). Therefore, depending on the injury that we are dealing with, we can use more specific RTP strength criteria to target the area of the injured muscle. Some tests could give as a better indication of the injured area’s function and its ability to cope with the high-intensity stimuli on the field of play.
Mechanism of injury
The risk of a hamstring injury is higher when reaching very high speeds during sprinting (which is the most common hamstring mechanism), but other movements can also cause the injury. The stretching type mechanisms can be divided into: a) open-chain stretch type injuries caused by an overstretch, likely in a combination of hip flexion and knee extension and b) closed-chain, likely during a movement that involves high eccentric forces in a lengthened position (7). The most appropriate criteria can also be defined based on the mechanism to reproduce and test the movement that caused the injury and the ability of the muscle to produce high forces in those specific and often lengthened positions.
Conclusion
When deciding on the RTP criteria following a hamstring injury in professional football, we should consider:
- The tissues involved and what is the best way to stress the injured structure.
- The area of injury because during muscle strength testing, each muscle area can be activate with a different testing position and movement.
- The mechanism of injury can direct our decision towards testing the athlete’s ability to complete the task and specifically target the muscle’s ability to contract in lengthened positions.
Authors:
Paolo Perna [1] and Marco Beato [1]
- School of Health and Sports Sciences, University of Suffolk, Ipswich, United Kingdom.
References
- Ekstrand J, Bengtsson H, Waldén M, Davison M, Khan KM, Hägglund M. Hamstring injury rates have increased during recent seasons and now constitute 24% of all injuries in men’s professional football: the UEFA Elite Club Injury Study from 2001/02 to 2021/22. Br J Sports Med. 2023 Mar;57(5):292–8.
- Kerin F, O’Flanagan S, Coyle J, Curley D, Farrell G, Persson UM, et al. Are all hamstring injuries equal? A retrospective analysis of time to return to full training following BAMIC type ‘c’ and T‐junction injuries in professional men’s rugby union. Scand J Med Sci Sports. 2024 Feb;34(2):e14586.
- Pollock N, James SLJ, Lee JC, Chakraverty R. British athletics muscle injury classification: a new grading system. Br J Sports Med. 2014 Sep;48(18):1347–51.
- Beattie CE, Barnett RJ, Williams J, Sim J, Pullinger SA. Are return-to-play times longer in lower-limb muscle injuries involving the intramuscular tendon? A systematic review. J Sci Med Sport. 2023 Oct;S1440244023004231.
- Bourne MN, Williams MD, Opar DA, Al Najjar A, Kerr GK, Shield AJ. Impact of exercise selection on hamstring muscle activation. Br J Sports Med. 2017 Jul;51(13):1021–8.
- Mendez-Villanueva A, Suarez-Arrones L, Rodas G, Fernandez-Gonzalo R, Tesch P, Linnehan R, et al. MRI-Based Regional Muscle Use during Hamstring Strengthening Exercises in Elite Soccer Players. Lucia A, editor. PLOS ONE. 2016 Sep 1;11(9):e0161356.
- Della Villa F, Massa B, Bortolami A, Nanni G, Olmo J, Buckthorpe M. Injury mechanisms and situational patterns of severe lower limb muscle injuries in male professional football (soccer) players: a systematic video analysis study on 103 cases. Br J Sports Med. 2023 Dec;57(24):1550–8.