This blog is part of a series on groin pain by Jim Scanlan, Physiotherapist. Keep an eye out for monthly releases in this series!
Diagnosing, managing & rehabilitating injuries in the Bermuda triangle
Keywords: Groin Pain; Adductor; Rehabilitation
Introduction:
Sports involving rapid acceleration, deceleration or sudden changes in direction commonly result in groin injuries (1). This includes football (soccer) (2), (3), (4), (5), (6), (7), (8), (9), (10), (11), (12) & (13); rugby league (14); Australian rules football (15); ice hockey (16); Gaelic football and cricket (16) & (17). Athletes with a previous groin injury are at a greater risk than those with no previous history (up to 2.4 times greater over consecutive seasons within football) (11). The diagnosis of groin injuries is complex with a multifactorial aetiology (18). This blog is the first in a series discussing some of these complexities, along with management and rehabilitation strategies. Beginning with adductor related groin pain (ARGP).
Adductor Related Groin Pain (ARGP):
ARGP is defined as adductor tenderness and pain on resisted adduction testing (see Figure 1) (18). ARGP has an incidence of between 3 and 23% (19), (20) & (21) more commonly affecting young to middle-aged athletic males compared to females. Certain sports, such as football, have a yearly incidence of 10-18% (21) with approximately 53% of ARGP within football being from overuse (22).
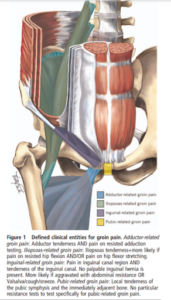
Figure 1: Groin Pain (Weir A, Brukner P, Delahunt E, et al, 2015) (18)
The Copenhagen ‘Hip and Groin Outcome Score’ (HAGOS) (23) is a patient reported outcome measure with six separate subscales, assessing pain; symptoms; physical function in daily living; physical function in sport and recreation; participating in physical activities and hip and / or groin quality of life. It has substantial test-retest reliability with adequate measurement qualities for use with physically active, young to middle-aged patients with long-standing hip and / or groin pain.
As defined by Weir et al. (2015) (18) ARGP was found to be the most common clinical entity (61% of athletes) (24) , with the vast majority of these athletes being male (98%) football (60%) players. There were multiple causes for the ARGP. Unfortunately study quality on groin injury management has been historically low (25). This could be because there is a close and complex relationship between ARGP and Pubic Related Groin Pain, along with other aspects of groin pain such as iliopsoas and inguinal.
The most efficacious treatment for long-standing ARGP is exercise therapy. There is insufficient evidence within the literature to recommend a specific exercise protocol or modality (19). However the exercises described in the modules from Hölmich et al (1999) (26) and iteration (27) appear to be beneficial, regarding reduction in pain and return to sport without groin pain at 16 week follow up in comparison to passive treatments (exercise stretching, electrotherapy and transverse friction massage). Emphasis should be paid to adductor eccentric strength in particular (27). Use of The ‘Copenhagen Adduction’ (CA) exercise (see Figure 2) reduced the prevalence and risk of groin problems in male footballers by 41% (28).
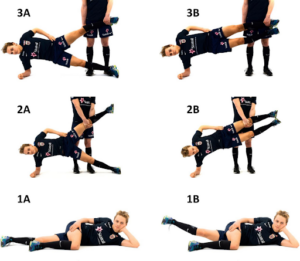
Figure 2: The Copenhagen Adduction Exercise (A) starting / ending position and (B) mid positions, for the different levels of the adductor strengthening programme (Haroy J, Clarsen B, Wiger EG, et al, 2019) (28)
Rehabilitation focused on inter-segmental control has been associated with improved HAGOS (23) scores and good rates of pain-free return to sport across (29) a variety of groin pain diagnoses (18).
SSC Sports Medicine Groin Lab – 180 Cut Series – YouTube (29)
For those patients wanting to return to sport the ‘Strategic Assessment of Risk and Risk Tolerance’ (StARRT) Framework, established in 2016 (30), is a good starting point for making return to play decisions post ARGP (see Figure 3).
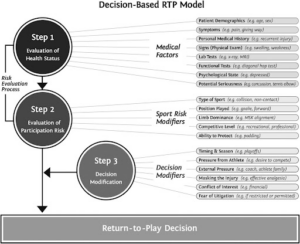
Figure 3 Strategic Assessment of Risk and Risk Tolerance Framework (Ardern CL, Glasgow P, Schneiders A, et al. 2016) (30)
Conclusions
- Groin pain has clearly defined clinical entities. Groin injuries are complex with a multifactorial aetiology.
- HAGOS is a valid tool to monitor long-standing groin pain rehabilitation.
- The most efficacious treatment for long-standing ARGP is exercise therapy.
Acknowledgements: Thank you to the Association Chartered Physiotherapists in Sports and Exercise Medicine @physiosinsport for their support in publishing this Blog.
Competing Interests: None
Jim Scanlan NHS Fife Advanced Practitioner Physiotherapist in General Practice
MSc; BSc (Hons); Pg Dip Orho Med; Pg Dip Injection Therapy; IRMER Certified;
HCPC; MCSP; ACPSEM: Silver Accreditation. Twitter: @jim_physio
References
(1) Whittaker JL, Small C, Maffey L, et al. Risk factors for groin injury in sport: an updated systematic review. Br J Sports Med 2015;0:1–8 DOI: https://10.1136/bjsports-2014-094287
(2) Werner J, Hagglund M, Walden M, et al. UEFA injury study: a prospective study of hip and groin injuries in professional football over seven consecutive seasons. Br J Sports Med 2009;43:1036–40. DOI: https://10.1136/bjsm.2009.066944
(3) Arnason A, Sigurdsson SB, Gudmundsson A, et al. Risk factors for injuries in football. Am J Sports Med 2004;32(1 Suppl):5S–16S. DOI: https://10.1177/0363546503258912
(4) Crow JF, Pearce AJ, Veale JP, et al. Hip adductor muscle strength is reduced preceding and during the onset of groin pain in elite junior Australian football players. J Sci Med Sport 2010;13:202–4. DOI: https://10.1016/j.jsams.2009.03.007
(5) Ekstrand J, Hagglund M, Walden M. Epidemiology of muscle injuries in professional football (soccer). Am J Sports Med 2011;39:1226–32. DOI: https://10.1177/0363546510395879
(6) Anderson DD, Chubinskaya S, Guilak F, et al. Post-traumatic osteoarthritis: improved understanding and opportunities for early intervention. J Orthop Res 2011;29:802–9. DOI: https://10.1002/jor.21359
(7) Ibrahim A, Murrell GA, Knapman P. Adductor strain and hip range of movement in male professional soccer players. J Orthop Surg 2007;15:46–9. DOI: https://10.1177/230949900701500111
(8) Witvrouw E, Danneels L, Asselman P, et al. Muscle flexibility as a risk factor for developing muscle injuries in male professional soccer players. A prospective study. Am J Sports Med 2003;31:41–6. DOI: https://10.1177/03635465030310011801
(9) Eirale C, Tol JL, Whiteley R, et al. Different injury pattern in goalkeepers compared to field players: a three-year epidemiological study of professional football. J Sci Med Sport 2014;17:34–8. DOI: https://10.1016/j.jsams.2013.05.004
(10) Engebretsen AH, Myklebust G, Holme I, et al. Intrinsic risk factors for groin injuries among male soccer players: a prospective cohort study. Am J Sports Med 2010;38:2051–7. DOI: https://10.1177/0363546510375544
(11) Hagglund M, Walden M, Ekstrand J. Previous injury as a risk factor for injury in elite football: a prospective study over two consecutive seasons. Br J Sports Med 2006;40:767–72. DOI: https://10.1136/bjsm.2006.026609
(12) Hagglund M, Walden M, Ekstrand J. Injuries among male and female elite football players. Scand J Med Sci Sports 2009;19:819–27. DOI: https://10.1111/j.1600-0838.2008.00861.x
(13) Paajanen H, Ristolainen L, Turunen H, et al. Prevalence and etiological factors of sport-related groin injuries in top-level soccer compared to non-contact sports. Arch Orthop Trauma Surg 2011;131:261–6. DOI: https://10.1007/s00402-010-1169-1
(14) O’Connor D. Groin injuries in professional rugby league players: a prospective study. J Sports Sci 2004;22:629–36. DOI: https://10.1080/02640410310001655804
(15) Orchard J, Wood T, Seward H, et al. Comparison of injuries in elite senior and junior Australian football. J Sci Med Sport 1998;1:83–8. DOI: https://10.1016/s1440-2440(98)80016-9
(16) Emery CA, Meeuwisse WH. Risk factors for groin injuries in hockey. Med Sci Sports Exerc 2001;33:1423–33. DOI: https://10.1097/00005768-200109000-00002
(17) Tyler TF, Nicholas SJ, Campbell RJ, et al. The association of hip strength and flexibility with the incidence of adductor muscle strains in professional ice hockey players. Am J Sports Med 2001;29:124–8. DOI: https://10.1177/03635465010290020301
(18) Weir A, Brukner P, Delahunt E, et al. Doha agreement meeting on terminology and definitions in groin pain in athletes. Br J Sports Med 2015;49:768-74. DOI: https://doi:10.1136/bjsports-2015-094869
(19) Almeida MO, Silva BNG, Andriolo RB, et al. Conservative interventions for treating exercise-related musculotendinous, ligamentous and osseous groin pain (Review). Cochrane Database of Systematic Reviews 2013;6. Art. No.: CD009565. DOI: https://10.1002/14651858.CD009565.pub2
(20) Bisciotti GN, Chamari K, Cena E, et al. The conservative treatment of longstanding adductor-related groin pain syndrome: a critical and systematic review. Biol Sport 2020;38(1):45-63. DOI: https://doi.org/10.5114/biolsport.2020.97669
(21) Mosler AB, Weir A, Eirale C, et al. Epidemiology of time loss groin injuries in a men’s professional football league: a 2-year prospective study of 17 clubs and 606 players. Br J Sports Med 2018;52(5):292–97. DOI: https://10.1136/bjsports-2016-097277
(22) Werner J, Hagglund M, Walden M, et al. UEFA injury study: a prospective study of hip and groin injuries in professional football over seven consecutive seasons. Br J Spots Med 2009;43(13):1036-40. DOI: https://10.1136/bjsm.2009.066944
(23) Thorborg K, Holmich P, Christensen R, et al. The Copenhagen Hip and Groin Outcome Score (HAGOS): development and validation according to the COSMIN checklist. Br J Sports Med 2011;45(6):478-91. DOI: https://10.1136/bjsm.2010.080937
(24) Taylor R, Vuckovic Z, Mosler A, et al. Multidisciplinary Assessment of 100 Athletes With Groin Pain Using the Doha Agreement: High Prevalence of Adductor-Related Groin Pain in Conjunction With Multiple Causes. Clin J Sport Med 2018;28(4):364-69. DOI: https://10.1097/JSM.0000000000000469
(25) Serner A, van Eijck CH, Beumer BR, et al. Study quality on groin injury management remains low: a systematic review on treatment of groin pain in athletes. Br J Sports Med 2015;49:813-24. DOI: https://10.1136/bjsports-2014-094256
(26) Holmich P, Uhrskou P, Ulnits L, et al. Effectiveness of active physical training as treatment for long-standing adductor-related groin pain in athletes: randomised trial. The Lancet 1999;353:439-43. DOI: https://10.1016/S0140-6736(98)03340-6
(27) Yousefzadeh A, Shadmehr A, Olyaei GR, et al. Effect of Holmich protocol exercise therapy on long-standing adductor-related groin pain in athletes: an objective evaluation. BMJ Open Sport & Exercise Medicine 2018;4:e000343. DOI: https://0.1136/bmjsem-2018-000343
(28) Haroy J, Clarsen B, Wiger EG, et al. The Adductor Strengthening Programme prevents groin problems among male football players: a cluster-randomised controlled trial. Br J Sports Med 2019;53:145-52. DOI: https://10.1136/bjsports-2017-098937
(29) King E, Franklyn-Miller A, Richter, C, et al. Clinical and biomechanical outcomes of rehabilitation targeting intersegmental control in athletic groin pain: prospective cohort of 205 patients. Br J Sports Med 2018;52:1054-62. DOI: https://10.1136/bjsports-2016-097089
(30) Ardern CL, Glasgow P, Schneiders, et al. 2016 Consensus statement on return to sport from the First World Congress in Sports Physical Therapy, Bern. Br J Sports Med 2016:50:853-64. DOI: https://10.1136/bjsports-2016-096278