Shoulder injuries are common in sport, especially amongst overhead throwing athletes who use their upper arm and shoulder in an arc over head to propel a ball toward the opposing team. Athletes in repetitive overhead sports such as volleyball, baseball, and softball are at high risk of injuring their superior labrum and acromioclavicular (AC) joint (1). Most of the reported shoulder issues are strains with chronic overload leading to an injury (2).
This blog provides an overview of how the O’Brien’s test can be utilized by medical doctors in the diagnosis of common shoulder injuries in athletes.
Common Shoulder Injuries in Overhead Athletes
Specifically, superior labrum, anterior and posterior (SLAP) lesions occur due to tears of the glenoid labrum fibrocartilage. The labrum provides support and stability to the shoulder along with the rotator cuff tendon and muscles.
Throwing activities can also place stress on the AC joint, a synovial joint that connects the collarbone and shoulder blade with coracoclavicular (CC) ligaments. An injury to the AC joint is commonly known as “shoulder separation” and can be classified into the following types:
- Type I = the AC ligament is slightly sprained, but there’s no damage to the CC ligament.
- Type II = the AC ligament is completely torn, and there’s a sprain or partial tear of the CC ligament.
- Type III = both the AC and CC ligaments are completely torn. In this case, the collar bone separates from the end of the shoulder blade.
- Type IV, V, VI injuries are the most severe as the clavicle becomes completely displaced.
Physical exams, such as the O’Brien’s test, can be a key procedure to identify and assess SLAP lesions and AC joint abnormalities.
What is the O’Brien’s Test?
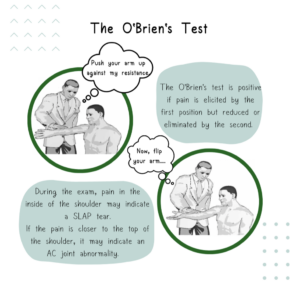
The O’Brien’s Test, also known as the Active Compression Test, was developed by Dr. Stephen J. O’Brien, MD, MBA, an orthopedic surgeon specialized in sports medicine, to evaluate labral tears and AC joint abnormalities (3). To perform the test, the patient is instructed to forward flex their arm to 90 degrees with their elbow in full extension, then adduct their arm 10-15 degrees medial to the sagittal plane of their body with palms pronated. While the patient stands in this position, the medical examiner applies a downward force on their arm and asks them to bring the arms upwards against their resistance. Then, the patient is instructed to repeat the same maneuver, but with their palms supinated. Again, the medical examiner applies a downward force on their arm and asks them to resist.
If the patient experiences pain during the first manoeuvre, but then experiences little or no pain in the second position, their O’Brien’s test is considered positive (3).
Figure 1 –– Illustrations adapted from Tennent et al. (2003) (4).
Validity of the O’Brien’s Test
Previous studies have examined the diagnostic accuracy of the O’Brien’s test, with specificity values ranging from 28-73% and sensitivity values ranging from 63-94% (5, 6). The literature suggests that no single physical examination maneuver is adequate for accurate diagnosis of SLAP tears and AC joint abnormalities. The O’Brien’s test is often combined with other tests like Speed’s and Yergason’s during an orthopedic examination of the shoulder. However, more studies are needed to understand the accuracy of the test amongst young athletes.
Next Steps
If the O’Brien’s test is positive, a physician will likely order an MRI (Magnetic Resonance Imaging) arthrogram to properly identify and diagnose the injury, whether it is a SLAP tear or AC joint abnormality. Once diagnosed, treatment will vary based on the type and extent of the injury.
Author information
Anika Nayak (anikanayak@berkeley.edu)
References
- Michener LA, Abrams JS, Bliven KCH, et al. National Athletic Trainers’ Association Position Statement: Evaluation, Management, and Outcomes of and Return-to- Play Criteria for Overhead Athletes With Superior Labral Anterior-Posterior Injuries. Journal of Athletic Training 2018;53:209–29. doi:https://doi.org/10.4085/1062-6050-59-16
- Cools AM, Johansson FR, Borms D, et al. Prevention of shoulder injuries in overhead athletes: a science-based approach. Brazilian Journal of Physical Therapy 2015;19:331–9. doi:https://doi.org/10.1590/bjpt-rbf.2014.0109
- O’Brien SJ, Pagnani MJ, Fealy S, et al. The Active Compression Test: A New and Effective Test for Diagnosing Labral Tears and Acromioclavicular Joint Abnormality. The American Journal of Sports Medicine 1998;26:610–3. doi:https://doi.org/10.1177/03635465980260050201
- Tennent TD, Beach WR, Meyers JF. A Review of the Special Tests Associated with Shoulder Examination: Part II: Laxity, Instability, and Superior Labral Anterior and Posterior (SLAP) Lesions. The American Journal of Sports Medicine 2003;31:301–7. doi:https://doi.org/10.1177/03635465030310022601
- Ebinger N, Magosch P, Lichtenberg S, et al. A New SLAP Test: The Supine Flexion Resistance Test. Arthroscopy: The Journal of Arthroscopic & Related Surgery 2008;24:500–5. doi:https://doi.org/10.1016/j.arthro.2007.11.017
- Guanche CA, Jones DC. Clinical testing for tears of the glenoid labrum. Arthroscopy: The Journal of Arthroscopic & Related Surgery 2003;19:517–23. doi:https://doi.org/10.1053/jars.2003.50104