Keywords: knee pain, osteoarthritis, opioids, physical therapy, exercise
In this blog, we explain the findings from our recent study on the relation of timing of physical therapy initiation after a diagnosis of knee osteoarthritis with risk of opioid use in the future (1).
Why is this study important?
Knee osteoarthritis (OA) is a leading cause of chronic pain and physical disability in middle- and older-age adults worldwide. Exercise and education, typically included as part of physical therapy (PT) care, are the recommended first-line treatments for people who get diagnosed with knee OA. However, PT remains extremely underutilized for management of arthritis pain and patients continue to be prescribed painkillers, including opioids. Hence, arthritis pain is a significant contributor to opioid prescriptions.
In this study, we examined whether early initiation of PT after knee OA diagnosis can reduce future risk of opioids. The information from this study can be used by healthcare providers, insurers, and patients to guide clinical decisions.
How did the study go about this?
We used insurance claims data from 1999-2018 for this study. We identified those diagnosed with knee OA and received PT within 1-year of the diagnosis. We then grouped the people into those who started PT < 1 month, 1- < 3 months, 3 – < 6 months, 6-< 9 months, and 9-12 months after the diagnosis. Over a 1-year period starting 1-year after the date of the diagnosis, we also determined whether these individuals were prescribed any opioids and if they were prescribed opioids long-term. We were then able to statistically compare the risk of any opioid use and long-term opioid use in people who started PT any time > 1-month after diagnosis with those who started PT < 1-month after diagnosis. For all these comparisons we accounted for other factors that could influence when a person starts PT care after diagnosis and if they use opioids. These included age, sex, race, obesity, type of insurance, location, physical and mental health conditions, prior healthcare utilization, and calendar year. For all analyses, we looked at people who had previously used opioids (opioid experienced) and those who had not used opioids before (opioid naïve).
What did the study find?
We identified 2,194,144 persons who were diagnosed with knee OA during the study period in the insurance database. Of these, 67,245 were included in this study based on the study criteria. Of these 35,899 were opioid naïve and 31,346 were opioid experienced. We found that a delay in initiation of PT after diagnosis was associated with a greater risk of future opioid use. The greater the delay, the greater the risk. This finding was true for both opioid naïve and opioid experienced persons and for both any opioid use and long-term opioid use.
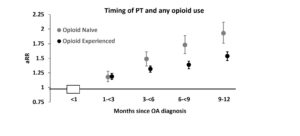
Figure 3: Timing of PT and any opiod use
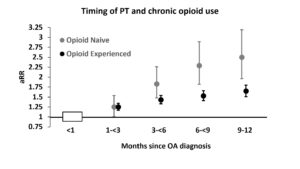
Figure 4: Timing of PT and chronic opiod use
What are the key take-home points?
The results from this large real-world study using data from a large and representative cohort of American adults show that among people who receive a diagnosis of knee OA and are referred to PT, those starting PT > 1-month after the diagnosis have greater risk of using opioids for their knee pain in the future. Hence, strategies to ensure early initiation of PT care are needed to reduce reliance on opioids. Expanded reimbursement of self-referral, telerehabilitation, and implementation of clinical practice guidelines, are some approaches to improve early access and referral to PT.

References
- Kumar D, Neogi T, Peloquin C, et al Delayed timing of physical therapy initiation increases the risk of future opioid use in individuals with knee osteoarthritis: a real-world cohort study British Journal of Sports Medicine Published Online First: 23 February 2023. doi: 10.1136/bjsports-2022-106044
- Long, H., Liu, Q., Yin, H., Wang, K., Diao, N., Zhang, Y., Lin, J. and Guo, A. (2022), Prevalence Trends of Site-Specific Osteoarthritis From 1990 to 2019: Findings From the Global Burden of Disease Study 2019. Arthritis Rheumatol, 74: 1172-1183. https://doi.org/10.1002/art.42089
- Yu D, Hellberg C, Appleyard T, et al. Opioid use prior to total knee replacement: comparative analysis of trends in England and Sweden. Osteoarthritis Cartilage 2022;30(6):815-22. doi: 10.1016/j.joca.2022.02.621
- Kolasinski SL, Neogi T, Hochberg MC, et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis & rheumatology (Hoboken, NJ) 2020;72(2):220-33. doi: 10.1002/art.41142
Authors of blog
Deepak Kumar 1,2, Tuhina Neogi 2, Christine Peloquin 2, Lee Marinko 1, James Camarinos 1, Kosaku Aoyagi 2,3, David T Felson 2, Maureen Dubreuil 2,4
- Department of Physical Therapy, Boston University, Boston, Massachusetts, USA
- Section of Rheumatology, Department of Medicine, Boston University School of Medicine, Boston, Massachusetts, USA
- Physical Therapy Program, The University of Texas at El Paso, El Paso, Texas, USA
- Visiting Scholar, Optum Labs, Eden Prairie, Minnesota, USA