This blog provides a summary of a recent national cohort study of over 400,000 US adults that identifies the minimum effective dose of aerobic and muscle-strengthening exercise.
Why is this study important?
Physical activity guidelines for health include both aerobic and strength components. Specifically, to optimize health, the World Health Organization (WHO) recommends adults engage in at least 2.5 hours of moderate-intensity aerobic physical activity (MPA; e.g., walking briskly), 1.25 hours per week of vigorous-intensity aerobic physical activity (VPA; e.g., jogging, running), or an equivalent combination of the two. The WHO also recommends muscle-strengthening exercise (MSE) at least 2 times per week targeting all major muscle groups [1].
Despite the known health benefits (such as living longer and better), over 1.4 billion adults do not meet the recommendation for aerobic physical activity (PA), and 70% of adults fail to meet the MSE recommendation [2,3]. Consequently, annual physical inactivity-related deaths and healthcare costs exceed 5 million and $67.5 billion, respectively [4,5] and the WHO has ranked physical inactivity as the 4th leading risk factor for mortality [6].
This suggests that current PA promotion efforts are largely ineffective, possibly because – (1) current PA targets appear unachievable from the perspective of the general public and/or (2) the endpoint (improving health) may not provide enough motivation to get the general public moving. Therefore, we sought to identify the minimum effective dose of aerobic PA and MSE for reducing the risk of death by all-causes. That is, what is the least amount of aerobic PA and/or MSE adults can participate in while still significantly reducing their risk of death?
How did the study go about this?
We used a cohort of 416,420 US adults who were followed over 18 years from the National Health Interview Survey (NHIS). Cox proportional-hazard models assessed the impact of MPA, VPA, and MSE on survival time while controlling for age, sex, race-ethnicity, income, education, marital status, survey year, smoking status, body mass index, and chronic conditions.
What did the study find?
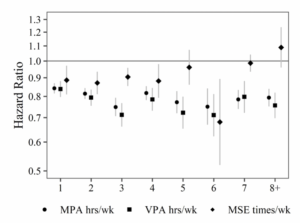
The first plot shows the independent impact of each hour per week of MPA and VPA, and each time per week of MSE, on mortality risk (vertical [y]-axis). Notice that MPA and VPA are associated with progressively decreasing mortality risk until ~3 hours per week. The inverse association between MSE and mortality risk was not significantly larger beyond participation in MSE more than 1 time per week.
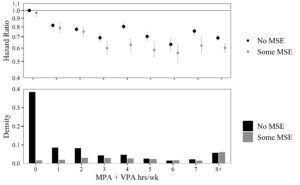
The second plot shows the combined impact of each hour per week of total PA (MPA + VPA) split by whether individuals did or did not participate in MSE. The top panel of the plot shows that MSE performed in addition to aerobic PA yielded the largest association with a decrease in mortality risk (the gray dots are generally lower than the black dots).
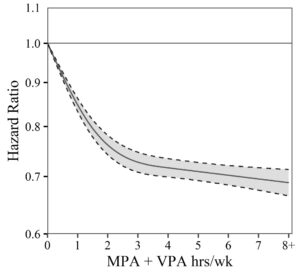
We used a nonlinear regression method to produce the third plot, which represents a simple illustration of a patient’s decrease in mortality risk as total PA increases. Notice that mortality risk decreases linearly as aerobic exercise increases but levels off at ~3 hours per week of MPA + VPA.
What are the key take-home points?
Adults should perform at least 1 hour per week of aerobic exercise (moderate and/or vigorous, whichever is more enjoyable and sustainable) to significantly improve health and reduce the risk of death by all-causes. We found little evidence that more than 3 hours per week of aerobic exercise yielded any additional benefits. Additionally, MSE performed 1-2 times per week independently improves health and reduces risk of death by all-causes and furthers health improvements gained from aerobic PA.
According to our findings, the optimal exercise regimen for reducing the risk of death by all-causes is 3 hours per week of aerobic exercise (moderate and/or vigorous) and 1-2 times per week of muscle-strengthening exercise (e.g., resistance training) targeting all 7 major muscle groups (legs, hips, back, abdomen, chest, shoulders, and arms).
Article reference:
Coleman CJ, McDonough DJ, Pope ZC, et al. Dose–response association of aerobic and muscle-strengthening physical activity with mortality: a national cohort study of 416 420 US adults. British Journal of Sports Medicine; 11 August 2022. https://doi.org/10.1136/bjsports-2022-105519
References
- Bull FC, Al-Ansari SS, Biddle S, et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br J Sports Med. Dec 2020;54(24):1451-1462.
- Guthold R, Stevens GA, Riley LM, Bull FC. Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys with 1·9 million participants. Lancet Glob Health. 10 2018;6(10):e1077-e1086.
- Bennie JA, Lee DC, Khan A, et al. Muscle-Strengthening Exercise Among 397,423 U.S. Adults: Prevalence, Correlates, and Associations With Health Conditions. Am J Prev Med. 12 2018;55(6):864-874.
- Ding D, Lawson KD, Kolbe-Alexander TL, et al. The economic burden of physical inactivity: a global analysis of major non-communicable diseases. Lancet. Sep 2016;388(10051):1311-1324.
- Ding D, Kolbe-Alexander T, Nguyen B, Katzmarzyk PT, Pratt M, Lawson KD. The economic burden of physical inactivity: a systematic review and critical appraisal. Br J Sports Med. Oct 2017;51(19):1392-1409.
- WHO. Global health risks: mortality and burden of disease attributable to selected major risks. World Health Organization. 2009; https://apps.who.int/handle/10665/44203. Accessed 24 November 2021.