Even More, Does It Really Matter?
Calf muscle injuries are common in sports involving high-speed running and specially in acceleration and deceleration actions. It has been reported that calf muscle injuries contribute about 13% of muscle injuries in football, though it may be that this percentage is even higher nowadays (1, 2).
It is easy and really common to speak about tennis leg (TL) injuries but, what is exactly a TL? It is a syndrome. It is defined as an acute pain in the postero–medial region of the calf with functional limitation. Most frequently, it is a medial gastrocnemious (MG) rupture, but it can also be a plantaris rupture or a soleus rupture(3). Another important aspect is to understand that an intermuscular hematoma is only one of the signs that we can see (NOT always) in TL syndrome.
Let’s focus on the most frequent injuries in the calf, the MG injuries.
Anatomy
One of the most important things is to understand the particular anatomy of the MG and the calf region. This region was well described by Blitz et al in 2007, summarised in figure 1.
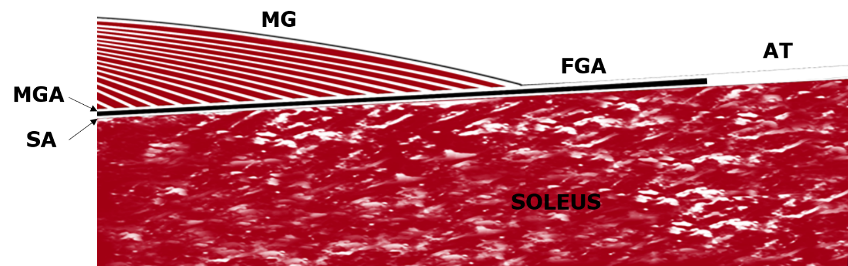
Fig. 1. Anatomical schema of the MG region. MGA (Medial Gastrocnemious Aponeurosis); SA (Soleus Aponeurosis); FGA (Free gastrocnemious Aponeurosis); AT (Achilles tendón).
What about Classifications and Imaging?
As is well known, there are in the recent years some important and interesting general muscle injuries classifications (5, 6). General classifications are really important but, in most cases, they don’t show the whole picture of what is happening in a specific area.
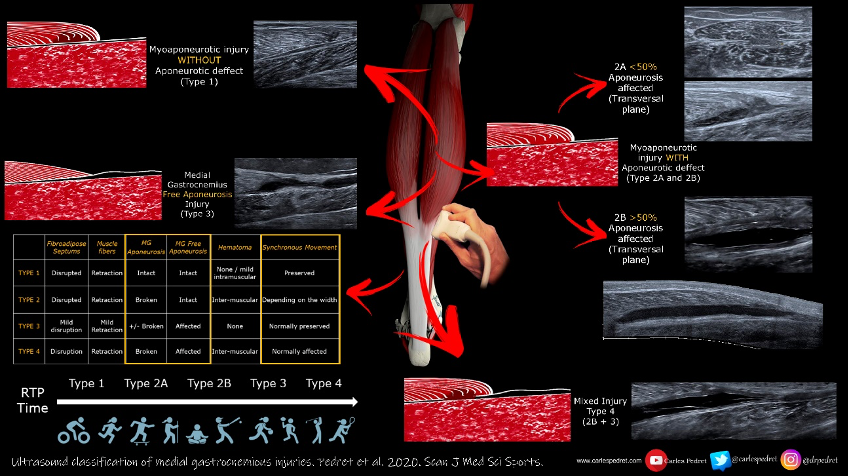
We realized, in recent years, that injuries affecting the MG had a great variety in their presentation and a highly variable prognosis despite occurring with the same injury mechanism and that all this could be seen easily with ultrasound. As such, we devised our own ultrasound classification system of medial gastrocnemious injuries.
115 subjects (64 athletes and 51 occupational workers )with an injury to the medial head of the gastrocnemius were divided in 5 MG injury types.
Ultrasound classification.
TYPE 1. Myoaponeurotic injury WITHOUT Aponeurotic deffect:
- MG / Soleus Aponeurosis: INTACT
- Fibroadipose Septums aspect: Retracted
- Muscle fiber aspect: Retracted
- Hematic suffusion: Between septum and aponeurosis
- Hematoma: None
- Synchronous Movement with plantarflexion and dorsiflexion of the ankle: PRESERVED
TYPE 2. Myoaponeurotic injury WITH Aponeurotic defect:
- MG / Soleus Aponeurosis: BROKEN
Type 2A: < 50% (in transversal ultrasound scan)
Type 2B: > 50% (in transversal ultrasound scan)
- Fibroadipose Septums aspect: Retracted
- Muscle fiber aspect: Retracted
- Hematic suffusion: Between septum and apon.
- Hematoma: Intermuscular (+/-)
- Synchronous Movement: Depending on the width of the aponeurosis rupture.
TYPE 3. Medial Gastrocnemius Free Aponeurosis Injury:
- MG / Soleus Aponeurosis: Free Aponeurosis affection.
- Fibroadipose Septums aspect: Quite Normal
- Muscle fibre aspect: Quite Normal
- Hematic suffusion: None or very mild
- Hematoma: None
- Synchronous Movement: Normally PRESERVED
TYPE 4. Mixed injury (Type 2B + Type 3).
The most interesting thing is that the longest return to previous activity periods were associated with injuries with FGA involvement (Type 3 and Type 4) and that intermuscular haematoma and Gastrocnemius-soleus asynchronous movement were observed when the injury affected >50% of the GA width.
Key points to take home.
- MG strain injury is the most frequent injury affecting the calf region.
- Ultrasound is the best imaging technique as it is easily accessible, cost-effective, and repeatable and Ii also offers the ability to perform dynamic manoeuvres to assess synchronous movement.
- 5 injury types are defined in this classification with different ultrasound patterns, characteristics and prognosis.
- This classification is easily and quickly applicable in daily clinical practice and can be very useful for the management of MG injuries.
Relevant twitter thread:
Hello, the unroll you asked for: @lorenzo_masci: if you missed the fantastic webinar on assessment and management of calf tears by @carlespedret then… https://t.co/9BzS85ebxZ Share this if you think it's interesting. 🤖
— Thread Reader App (@threadreaderapp) November 2, 2020
Author and Affiliation:
Dr Carles Pedret
Sports Medicine and Sports Orthopedics MD, PhD. Musculoskeletal sonographer
References:
- Bengtsson H, Ekstrand J, Hägglund M. Muscle injury rates in professional football increase with fixture congestion: an 11-year follow-up of the UEFA champions league injury study. Br J Sports Med 2013;47:743–7.
- Hägglund M, Waldén M, Ekstrand J. Risk factors for lower extremity muscle injury in professional soccer: the UEFA injury study. Am J Sports Med 2013;41:327–35.
- Delgado GJ, Chung CB, Lektrakul N, et al. Tennis leg: clinical US study of 141 patients and anatomic investigation of four cadavers with MR imaging and US. Radiology. 2002 Jul;224(1):112-9.
- Blitz NM, Eliot DJ. Anatomical aspects of the gastrocnemius aponeurosis and its insertion: a cadaveric study. J Foot Ankle Surg. 2007;46(2):101-108.
- Pollock N, James SLJ, Lee JC, et al. British athletics muscle injury classification: a new grading system. Br J Sports Med. 2014;48(18):1347-1351.
- Valle X, Alentorn-Geli E, Tol JL, et al. Muscle injuries in sports: a new evidence-informed and expert consensus-based classification with clinical application. Sport Med. 2017;47(7):1241-1253