Ben Jones 1,2,3,4,5, Gemma Phillips 2,6, Simon PT Kemp 7,10, Steffan A Griffin 7,8, Clint Readhead 4,9, Neil Pearce 10, Keith A Stokes 7,11
Background
The COVID-19 pandemic has resulted in global disruption to many sports. There are a number of challenges in returning to sport, especially given the unprecedented duration of time that athletes have not been able to train or compete in normal environments(1), the potential health risk to athletes, their coaches, support staff, the wider public, and the limited evidence base available to inform decisions. Every sport will carry different infection risks, given the specific match demands and training requirements(2). Furthermore, considerations regarding the return to training and match play will be greatly influenced by the national impact of COVID-19(3). A good example is the comparison of United Kingdom (COVID-19 mortality of >42,000), vs. Australia and New Zealand (COVID-19 mortality of <150)(4). In particular, New Zealand has now eliminated SARS-CoV-2, and rugby and other sports are now occurring ‘as normal’.
Quantifying the Risks of Sports during the COVID-19 Pandemic
A challenge in the current COVID-19 landscape is the lack of detailed understanding of the interplay of the factors influencing viral transmission, which is needed when considering the nuances of risk for exercising individuals in a sporting context. Quantifying and reducing activities which result in a greater potential for SARS-CoV-2 exposure, should an infected player participate, is a key control measure to prevent the spread of the disease. A granular understanding and description of an individual’s exposure is required if other players need to isolate, should a player test positive. Sports are following a phased return employing risk assessment and mitigation strategies that include using symptom checklists, implementing strict hygiene measures, following social distancing guidelines, modifying training progressions and many also include enhanced testing programmes for all players(5). Collectively these will likely reduce the risk of a player who has COVID-19 participating in training or match play. Given the acknowledged limitations of testing(6) (i.e., there is currently a 30% chance of a false-negative test result(7)) the existence of asymptomatic infections, or because of the duration of time between testing, a player may inadvertently participate whilst ‘carrying’ COVID-19, and therefore may expose team mates, opposition and the wider community to the virus.
Commercially available technology (e.g., GPS) allows the quantification of proximity between players(8) to estimate the potential risk of SARS-CoV-2 exposure, based on predetermined thresholds (e.g., 1 – 3 m(9)). This is useful for wider proximity breaches (e.g., 2.5 ± 1 m(10)), but closer interactions may be harder to determine, which are important given face-to-face encounters appears the highest risk.
Team Sport Risk Exposure Framework
To support the safe return to sport, a decision-making framework to provide structure and consistency when considering the risk of virus transmission for team sports, may be useful, even if the parameters (e.g., player proximity, duration of proximity breach) change with the emergence of sport specific evidence and guidance. As such, we propose the Team Sport Risk Exposure framework (Figure 1) to guide decisions around possible law change, non-law driven player behaviour change, training practice modifications, and discussions around the Public Health led sport-specific ‘test and trace’ process to determine individual risk for potential case contacts (should a squad or support staff member test positive with COVID-19). The framework considers proximity, accumulative proximity exposure and the frequency and duration of face-to-face exposure. It defines thresholds for fleeting and non-fleeting exposure and proposes an accumulative threshold of 15 minutes for medium risk activities that take place outdoors. It proposes that this threshold be reviewed for indoor / low ventilation environments based on risk assessments.
Low risk activities are defined as low risk of SARS-CoV-2 exposure (determined by degree of player proximity), and unlikely to become an increased-risk activity with increased exposure (duration of close proximity). Medium risk activities are defined as low risk of SARS-CoV-2 face-to-face exposure, but with some chance of becoming increased risk with greater exposure. Increased risk activities are defined as those with higher risk of SARS-CoV-2 exposure between players.
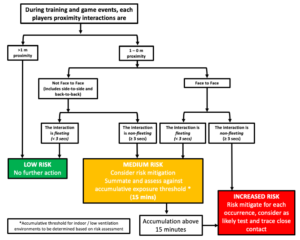
Figure 1. The Team Sport Risk Exposure Framework
Applying the Team Sport Risk Exposure Framework in practice – A Case Study using Rugby League
The specific application of the Team Sport Risk Exposure framework to rugby league match play is shown in Figure 2. The fundamental actions of rugby league and their interactions are depicted (Figure 2a), then using the Team Sport Risk Exposure framework, each activity is assigned a rating of ‘increased, medium and low risk’ (Figure 2b). Rule and player behaviour interventions may be able to ‘downgrade’ the classification assigned to individual activities or remove these activities (Figure 2c).
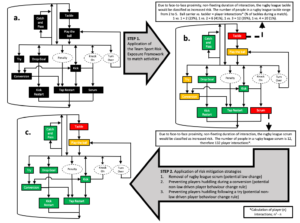
Figure 2. a) A list of rugby league game-specific actions b) Application of Team Sport Risk Exposure framework c) Rugby league game-specific actions following potential risk-reduction interventions
The Team Sport Risk Exposure framework can also be used to support the categorisation of increased, medium and low risk activities for the purposes of planning training progressions that balance performance enhancement and injury risk reduction in preparation for competition(1) against infection risk mitigation. Systematic classification of the risk of different activities forms part of the infection risk assessment process. Different approaches can be taken to assessing infection risk in training. Table 1 shows the results when, (i) asking elite coaches to rate infection risk after viewing footage of training sessions, (ii) calculating time that players spend within 2-m proximity using GPS, (iii) calculating exposure to increased risk activities from video footage, and (iv) employing the Team Sport Risk Exposure framework. All methods provided similar risk classification, with the exception of one training session in which two player roles (lineout jumper and the player facing them to lift them) were deemed to be at medium risk using video analysis and the framework, with all other players at low risk.
Table 1. Application of the Team Sport Risk Exposure Framework to Training Activities
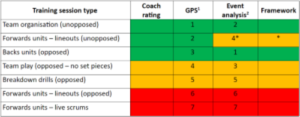
1 Numbers reflect ranking from low (1) to high (7) of the 2-m incursion time within a session
2 Numbers reflect ranking from low to high of increased risk events per minute of ball-in-play time
*Medium risk determined for the player jumping for the ball and the player facing them and lifting them. Risk for all other players rated as low.
Conclusion
Whilst the calculation of player interactions is likely an oversimplification of SARS-CoV-2 exposure and sources of COVID-19 transmission, given the current challenges, the Team Sport Risk Exposure framework does provide stakeholders with a practical method to inform discussions around the return-to-sport, law changes and non-law driven player behaviour change rules and training practice modifications as well as a possible route map through the sporting environment element of the contact tracing process following the identification of a positive case.
References
- Stokes, K. A., Jones, B., Bennett, M., Close, G. L., Gill, N., Hull, J. H., Kasper, A. M., Kemp, S., Mellalieu, S. D., Peirce, N., Stewart, B., Wall, B. T., West, S. W., & Cross, M. (2020). Returning to Play after Prolonged Training Restrictions in Professional Collision Sports. International journal of sports medicine, 10.1055/a-1180-3692. Advance online publication. https://doi.org/10.1055/a-1180-3692
- Whitehead, S., Till, K., Weaving, D., & Jones, B. (2018). The Use of Microtechnology to Quantify the Peak Match Demands of the Football Codes: A Systematic Review. Sports medicine (Auckland, N.Z.), 48(11), 2549–2575. https://doi.org/10.1007/s40279-018-0965-6
- Pearce N, Lawlor L, Brickley E. Comparisons between countries are essential for the control of COVID-19. International Journal of Epidemiology, in press.
- Max Roser, Hannah Ritchie, Esteban Ortiz-Ospina and Joe Hasell (2020) – “Coronavirus Pandemic (COVID-19)”. Published online at OurWorldInData.org. Retrieved from: ‘https://ourworldindata.org/coronavirus’ [Online Resource]
- Kemp S, Cowie C, Gillet M et al. Working with Government to plan a ‘return-to-sport’ during the COVID-19 pandemic: The United Kingdom’s collaborative 5-Stage model. Br J Sports Med 2020, In Press.
- Pearce N, Vandenbroucke J, VanderWeele T, Greenland S. Accurate Statistics on COVID-19 are essential for Policy Guidance and Decisions. American Journal of Public Health 2020; 110: 949-951.
- Watson, J., Whiting, P.F., Brush, J.E. Interpreting a covid-19 test result. BMJ 2020; 369: m1808
- Knudsen, N.S., Thomasen, M.M.D., Andersen, T.B., (pre-print). Spread of virus during soccer matches. doi: https://doi.org/10.1101/2020.04.26.20080614
- Chu, D. K., Akl, E. A., Duda, S., Solo, K., Yaacoub, S., Schünemann, H. J., & COVID-19 Systematic Urgent Review Group Effort (SURGE) study authors (2020). Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: a systematic review and meta-analysis. Lancet (London, England), S0140-6736(20)31142-9. Advance online publication. https://doi.org/10.1016/S0140-6736(20)31142-9
- Catapult Proximity Project: Incursion Validation Trials. Blog Published 12/06/2020. Available from: https://proximity-validation.catapultsports.com
Affiliations
1 Carnegie Applied Rugby Research (CARR) centre, Carnegie School of Sport, Leeds Beckett University, Leeds, UK
2 England Performance Unit, The Rugby Football League, Leeds, UK
3 Leeds Rhinos Rugby League club, Leeds, UK
4 Division of Exercise Science and Sports Medicine, Department of Human Biology, Faculty of Health Sciences, the University of Cape Town and the Sports Science Institute of South Africa, Cape Town, South Africa
5 School of Science and Technology, University of New England, Armidale, NSW, Australia.
6 Hull Kingston Rovers, Hull, UK
7 Rugby Football Union, Twickenham, UK
8 Centre for Sport and Exercise, University of Edinburgh, Edinburgh, UK
9 South African Rugby Union, SARU House, South Africa
10 London School of Hygiene and Tropical Medicine, London, UK
11 University of Bath, Bath, UK