By Dr Irfan Ahmed @Irfan_sem
As a sports medicine registrar I often get asked the question: what do you actually do?
The question is usually accompanied by a puzzled look (intrigue, I imagine) and a proposal that it’s a bit like “conservative orthopaedics”. After years of attempting different responses, including passionate descriptions of musculoskeletal (MSK) medicine and mission statements from the faculty; I felt as though I had made some progress in explaining it well! What I hadn’t expected –as a new Sports and Exercise Medicine Trainee (ST3) working at Charing Cross Hospital Emergency Department (ED)– was to start to ask myself that very same question!
In theory, the ED provides direct access to investigation and assessment, but given that 7.7% of all injury related ED attendances are a direct result of taking part in a sport1; it is a challenge to identify those acute injuries that would benefit from urgent assessment by a Sports and Exercise Medicine (SEM) physician2.
Using infographics to attract a new audience.
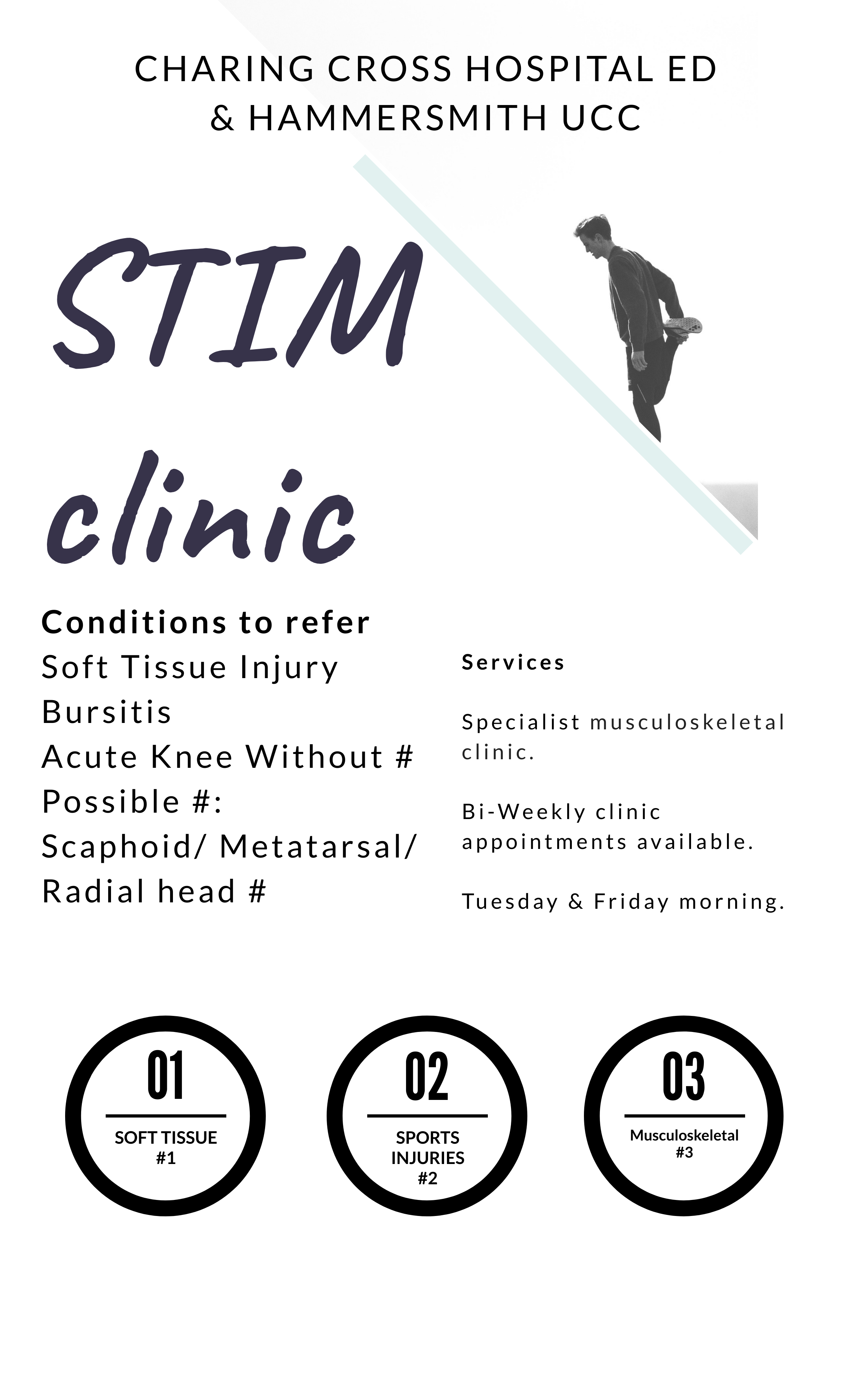
Keen to make a positive impact, I started to re-design the Soft Tissue, Injuries and Musculoskeletal (STIM) clinic from the ground up, one infographic at a time. As a trainee, this is your learning ground: injuries that often are “lost to follow up”, return for clinical review and a specialist SEM opinion in the ED. Tendinopathies, tender scaphoids, rotator cuff, ligament, muscle and acute knees injuries are the staple of the STIM clinic (Figure 1).
When working optimally, the STIM clinic gives patients more time and a chance to be analysed in depth, not just for their diagnosis but also to help the patient understand how they got injured in the first place as well as how they can avoid the injury in future. By bringing patients back for review, the STIM clinic helps to reduce the burden on the fracture clinic and primary care where 30% of all consultations are due to a musculoskeletal condition3.
The role of exercise & rehabilitation
Having been “Ottawa ankle rules positive” myself once in an A&E department, I know what it feels like first hand to be a patient caught in the “soft tissue gap”. Getting the all clear by a physician, is usually the end of most treatment plans in medicine, but for MSK injuries a “no fracture, discharge” is often the start of the journey. Well before patients return to competition they will have to clear early, middle and late stage ankle rehab protocols4, with the aim to assist a successful and sustained return to play5.
By the time patients attend the ED, more often than not the acute problem is underlined by a more chronic issue. However, when given the options of surgery, injections or exercise therapy with equal emphasis; it is exciting to see so many patients with common conditions such as achilles tendinopathy tend to opt for Alfredson’s rehab protocol over an invasive procedure6.
Integrated musculoskeletal care – a model for expansion.
The STIM clinic sits side by side with the fracture clinic and is based around the principle of a one-stop-shop; see and treat on the same day. With direct access to bloods tests, x-ray, point of care ultrasound, MSK radiologists and MRI, the clinic is well resourced. By working in collaboration, and as part of the musculoskeletal MDT, the clinic has been able to reduce time from injury to diagnosis, and ensures that patients start rehab in a timely way (Figure 2).
The “soft tissue gap” is a unique and challenging opportunity for SEM’s clinicians. Often patients with a sports injury are lost to follow up or present late at secondary care MSK clinics. By providing an integrated musculoskeletal service at the front door of the Emergency Department, we are able to demonstrate a patient-centred and cost-effective approach to sports injuries management. So, in response to those quizzical looks, I can say “in addition to creating infographics for the clinic, I work to streamline care- while keeping the patient a priority”.

***
Competing interests
None declared
Dr Irfan Ahmed (T: @Irfan_sem) is a Sport and Exercise Medicine (SEM) registrar (ST4) in London and continues to work as a General Practitioner. Dr Ahmed first developed his interest in SEM at university as a keen amateur boxer and continue to provide match day cover for sporting events. He is involved in teaching, and his current research interest is looking at the impact of mouthguards on athletic performance. Email: irfan.ahmed5@nhs.net
References
- NHS Digital. Accident and Emergency Attendances in England – 2014–15. See https://digital.nhs.uk/catalogue/PUB19883
- Malliaropoulos N, Ghrairi M, Zerguini Y, Padhiar N. Soft tissue injuries are still a challenge in musculoskeletal sports and exercise medicine. British Journal of Sports Medicine. 2016;50(24):1487-1487.
- Margham T. Musculoskeletal disorders: time for joint action in primary care. British Journal of General Practice. 2011;61(592):657-658.
- Janssen K. Infographic: Ankle sprain treatment and prevention timeline. British Journal of Sports Medicine. 2017;52(15):953-954.
- Clanton T, Matheny L, Jarvis H, Jeronimus A. Return to Play in Athletes Following Ankle Injuries. Sports Health: A Multidisciplinary Approach. 2012;4(6):471-474.
- Morrey B. A 5-year follow-up study of Alfredson’s heel-drop exercise programme in chronic midportion Achilles tendinopathy. Yearbook of Orthopedics. 2012;2012:310-311.