By Dr Scott Lear
With each passing week, we’re inundated with information regarding what to eat, what not to eat, when to eat and the latest diet trends. Do we aim for macronutrients, calories or food patterns? New studies come out either telling us what we know or that we’ve had it wrong all this time, while others seem to go around in circles telling us what was once good is bad and vice versa. Take the controversy around fat. For decades we were told to avoid eating fats, now, we’re not so sure if eating fats is good or bad.

If we add in commercial motives of the food industry it gets even more confusing (what is gluten-free water anyway?) and stealth marketing (there’s a reason why sugary cereals are on the lower and middle selves of grocery stores), and it’s enough to make us give up. I’m married to a dietitian and have been researching health living for decades and my head still spins thinking about it.
It’s not that scientists (like me) are trying to pull the wool over everybody’s heads (although studying something in which it is hard to ever come to a definitive conclusion is a great way for a scientist to continue to have work). It’s just that studying nutrition is extremely difficult.
A number of things make it difficult to understand what ideal nutrition is. Probably the number one complexity that we can’t change is that we need food to live. It’s not like smoking in which the ideal number of cigarettes smoked is zero. So we can’t just tell people what not to eat (which unfortunately happens). In addition, we need a variety of foods to live and thrive. We can’t survive for very long on one type of food.
Another issue is trying to find out what a person eats. Of course we can ask people what they eat, and people are usually pretty good but not exact. Last night our family had hamburgers for dinner; mine had cheese, lettuce, tomatoes, cucumber and ketchup and my son’s had cheese, ketchup and BBQ sauce. But it’s quite possible that people may just say they had a hamburger. It’s also hard to know how much a person ate. Most mornings I have a bowl of cereal, but I don’t know what size it is.
Some studies ask participants to measure out their food, which can help, although most people when measuring out their foods will actually change how much they eat (usually people measuring their food eat less). The dilemma in nutrition research is that the more accurate we get in measuring a person’s usual diet (using measuring cups, scales, portion samples), the more likely they are to change their diet. There might be some improvement in accuracy by using mobile phones but just asking people to record what they eat can change what a person eats. When I was doing a food diary, I would be lazy and not have a snack because I didn’t want to write it down.
Some studies look at adding or removing a certain food to a diet and how that relates to health outcomes like heart disease and death. For example, studies of fish intake suggest a lower risk of heart disease. But does it? When people eat fish, they may be eating less of something else to accommodate it (most often people eat less red meat when eating fish). So is it eating the fish that’s good, or not eating something else, or a bit of both?
A good example of this is the recent excitement around saturated fats with some studies saying they aren’t as bad as we thought. But really, it matters what we replace the fat with that is as important. If someone reduces their saturated fat and replaces it with sugars, this is most commonly a poor health change. However, if saturated fat is replaced with unsaturated fat, this could be a healthier choice.
Studying a new diet that requires people to change what they are eating is equally if not more challenging; change is hard, so adherence to a new study diet is usually low. For most people, taste and cost are the two biggest reasons to eat what they eat. Layer onto to that cultural and social meanings of food and nutrition is quite low on the list. Sometimes researchers will provide participants with foods, which can help minimize barriers to dietary changes and control what people eat. These studies are great at telling us how diets work but don’t really reflect real-world conditions where one has to buy and prepare their own food.
It is unlikely that science will ever provide the answer to: What is the ideal diet? There are too many factors and many more that I haven’t mentioned (for example: getting vitamins as a supplement compared to in its natural food state, do foods act differently in certain combinations). Add to the fact that we are all individuals and what may be ideal for one person, may not be for another.
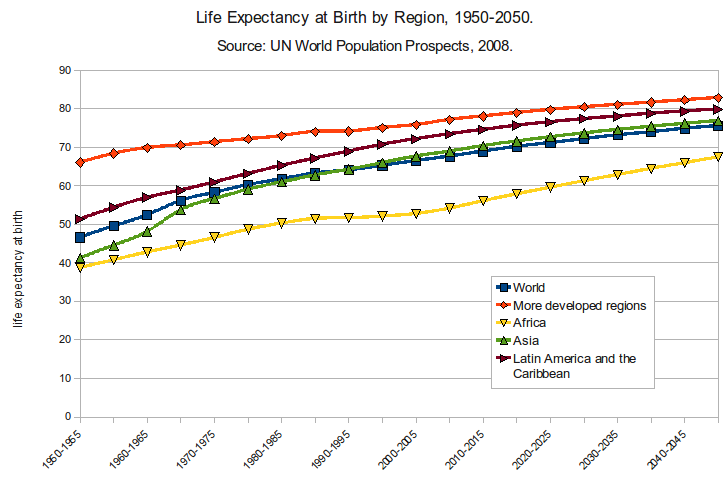
Despite the possible confusing and contradictory diet and nutrition advice, life expectancies around the globe continue to increase and a key reason for that is increased access to healthy foods. Even though we aren’t all nutrition scientists, we do have a pretty good understanding of what are healthy foods and our bodies are pretty good at metabolising the foods we eat.
{kind=link}
Where nutrition science comes in, regarding individual diet and nutrition, is it can help to delay the onset of disease and potentially add a few more quality years to our life that might not otherwise happen. This is a good thing, and we need to encourage health care professionals and scientists to provide this information in a way that makes it easily digestible (bad pun!).
In future blogs I’ll look to untangle some of the current nutritional controversies and how this may affect the food we eat.
Dr. Scott Lear is a Professor in Health Sciences at Simon Fraser University and holds the Pfizer/Heart and Stroke Foundation Chair in Cardiovascular Prevention Research at St. Paul’s Hospital. He is living with heart disease and writes this blog from his experience as both a researcher and patient.
This blog was reposted from Dr Lear’s blog, FEEL HEALTHY WITH DR. SCOTT LEAR.