By Nicol van Dyk, Physiotherapist, Rehabilitation Department, Aspetar Orthopaedic and Sports Medicine Hospital and;
Rod Whiteley, Assistant Director, Rehabilitation Department, Aspetar Orthopaedic and Sports Medicine Hospital
(presented at the ASICS Sports Medicine Australia conference 2015 – find all the slides here)
“It’s tough to make predictions, especially about the future.” Yogi Berra
It is still one of the most difficult questions clinicians have to answer: “When can I play again?” Not only the player, but also the coach and/or family members will push you for an answer. And then we all rub our crystal ball, get out the magic wand, and give them something we feel is sort of close to the mark. But in reality, we still have very little on which to base our predictions. Most of the time we’re guessing. (Educated guessing maybe, but guessing nonetheless.) But before that happens, we first have to get them through the rehab. Rehabilitation has moved away from time, and grown into criteria-based progression – the paradigm has begun to shift.
There are many excellent rehabilitation protocols of course, and you can find some of them in landmark papers such as Sherry and Best 2004. Reurink et al published an updated SR investigating different interventions for hamstring strain injury rehabilitation. Not wanting to be left out, we developed a hamstring rehabilitation protocol at the Aspetar Orthopaedic and Sports Medicine Hospital, based on available literature and clinical experience (that magic combination that doesn’t always like each other, but oh how sweet when they do). Our initial assessment and treatment includes elements that will form part of most protocols. So I will focus on three critical elements that we were able to identify:
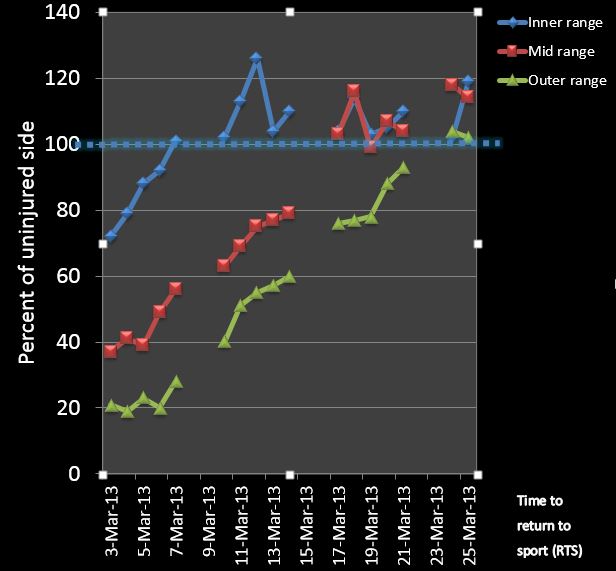
- The most important measurement is strength, especially outer range strength
- A running progression protocol that includes volume, intensity, mechanics, and is sport specific
- Criteria based progression between different stages in the rehabilitation
First things first – measure the strength.
With the use of standardized measurement procedure using hand held dynamometers, we measure inner, mid, and outer range strength of the injured and uninjured hamstring muscles. The most valuable measurement has been the outer range strength, as this has tracked well with return to play. In other words, by the time the player was discharged, he had regained his outer range strength fully when compared to the uninjured side. Mid-range strength was also tracking well, while inner range strength normalized much more quickly – often as fast as a few days, so it was less helpful to measure if your aim was to get a “progress bar” for this athlete’s rehabilitation. (Video of how to do this testing). We were fortunate to see patients 5 days a week, but if that is not possible, use the outer range strength measurement to keep track of the progression.
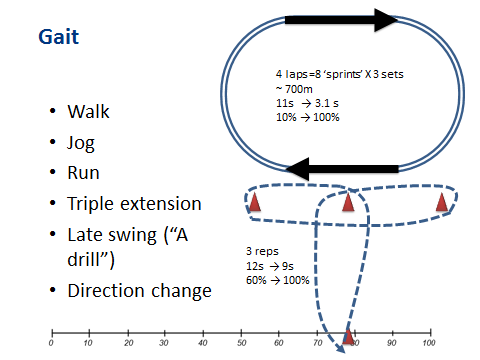
In our experience, nearly all of the hamstring injuries were due to running. If you see dancers (and maybe martial artists) you probably need to take our advice with a grain of salt. We agree with Askling that stretch type injuries are a different beast, but we can’t help you there as we really hardly ever see these. However for our patients, all rehab protocols must include running. Specifically, running as close as you can get to what would be required of the player and their sport. At our facility, players would typically run from stage 2 and run 3 sets of 4 laps on an indoor track (8 “sprints”) approximating 700m. We asked the player to rate their running on a scale from 0-100%, and timed their running. This was also an excellent way to keep track of their progression (another great tip if you don’t have running facilities or can’t see your patient daily). Finally, in stage 3 we included direction changes by modifying the T-drill a bit (in our version, keep running forwards, but with direction changes to run around the markers).
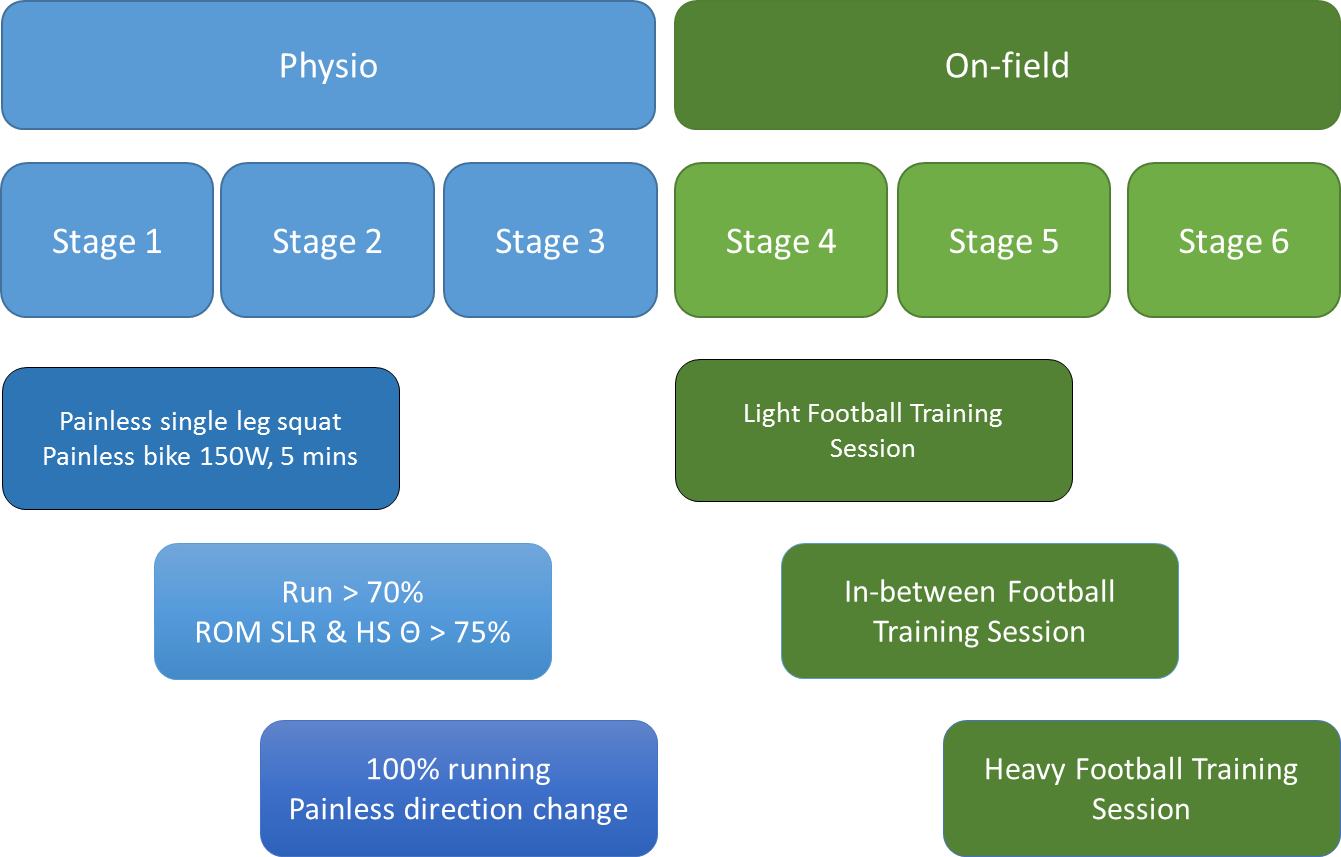
When the player was able to run at 100%, and do direction changes at 100%, he/she was allowed to go out on the field and perform sport specific rehabilitation with our sports rehabilitators. After they successfully complete 3 sessions, each one harder than the last, we performed some discharge tests (including isokinetic testing) and recommendations to the club to allow a gradual return to play.
Here is our criteria based progression algorithm:
And now, the magic question – when are they ready? Considering the outcome reported in the literature, it varies considerably. One thing we do know is that MRI parameters cannot help us to determine return to play, and adds no value above our clinical assessment. See this article by Arnlaug Wangensteen, who has contributed enormously to our rehabilitation programme.
So why is the outcome for return to sport so variable? Here’s a thought – perhaps because everyone is employing “conventional rehab” for their control groups, but no one knows what that is? In a soon to be published article in BJSM by Philipp Jacobsen, with some excellent work by co-author Rod Whiteley, they have investigated the things that we measure, and found some clinical predictors of return to play. So you will have to wait for the full length version to appear in an upcoming addition of BJSM, but here is the teaser:
Using a regression analysis, a combination of features you can easily measure in your clinical examination on day 1 and day 7 the week 1 examination could predict return to play within a 10 day window, explaining 97% of the variance! And here are the more important parameters to look out for:
- Length of pain on palpation
- Single leg bridge
- Hamstring strength (compared to the uninjured side) and whether it is painful or not
- Change in outer range strength over the week
Now, the data is over-fitted (which means it is too good to be true, and won’t stand up when they finish their replication study that’s nearly half way done), but even with that said, how good is a 10 day window? The coach, the player, the media – they want to know if the player will be ready for the final, and maybe now we can be confident ± 5 days. That is a pretty specific time point, and the reality is, even when I am using an equation set up to win, the best I can do is “Uh, yes, plus or minus 5 days.” Is that good enough? I have a sneaky suspicion that it will still not satisfy. But for now, it’s the best we can do!
So the next time you’re faced with the all impossible question, perhaps you have some better answers. Not easy answers, but we can say it will take about 3 weeks (give or take 5 days); we have a really good rehabilitation plan, which is measuring what you can do and your progression is based on that; and we will keep track of your progression based on what you need to return to play.
That’s probably as good as it gets!