By Steffan Griffin (@lifestylemedic) and Dr. Sean Carmody (@seancarmody1)
You may have seen @BJSMPlus – our conference twitter handle feeding various clinical pearls from events around the world – going into overdrive at the recent ‘Concussion: Diagnosis and Rehabilitation’ conference at the Sports Surgery Clinic in Dublin early last month #sscConcussion
This fantastic event, expertly organised by Colm Fuller and the rest of the team at SSC not only provided teaching from some of the world’s premier concussion experts, but also raised some intriguing questions and stimulated some great debate. Additionally, the conference provided an ideal opportunity to launch the innovative Post Concussion Rehabilitation Pathway that aims to improve the recovery process in concussed athletes.
In case you missed out – below are some highlights and impactful tweets – enjoy! All of the day’s stats are easily accessible via the 2012 Zurich Consensus Document, a must-read: http://bjsm.bmj.com/content/47/5/250.full
The Athlete’s Perspective Ruby Walsh
It was, perhaps, appropriate that a conference on Concussion was opened by horse-racing legend, Ruby Walsh. As Prof Paul McCrory and Dr Michael Turner later informed us, horse racing is the most high risk sport for developing concussions. During his talk, Ruby ignited a theme which was to recur throughout the day – “Concussion is not a new story and the media storm does not mean it’s a new issue, it’s simply in the news more often”.
Concussion Management – New Ideas and Global Consensus Professor Paul McCrory PhD
- We need to resort to scientific evidence and not media speculation when considering all aspects of a concussion – a culture of fear exists which may be unfounded.
- An example of this is the issue of suicide amongst NFL footballers in the USA – “Rate of suicide in 3049 retired NFL footballers (who played > 5 seasons) is 40% of age-matched non-footballers” – meaning that sport may confer a protective effect!
- At the moment – scans don’t rule in concussion, only rule out more serious pathologies
- Second Impact Syndrome should be called Single Impact Syndrome- there doesn’t have to be a second impact
- Examples of how concussions can be prevented include: coaching (eg tackle technique in collision sports), neck muscle strengthening, and rule changes (eg NFL rule banning hits with the crown of the helmet).
- Mouth guards have no role in preventing concussion.
- Our understanding of the pathogenesis of concussion is still very rudimentary. Do we know all of the causative pathways? Do NSAIDs put you at increased risk?
- The Mild/Moderate/Severe classification of concussion is inadequate in comparison to most other conditions. Breast cancer, for example, is classified according to clinical features, histological findings, hormonal receptor status and evidence of metastases- concussion has a long way to go.
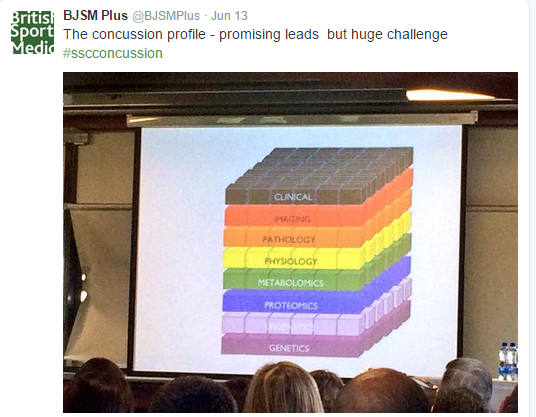
- Concussion has a wide and varied profile, with aspects stretching across many different clinical realms – it means that there is unlikely to be a single diagnostic test.
Taking a Targeted Approach to Concussion Rehabilitation Professor Willem Meeuwisse MD, PhD
- Normal recovery is dependent on age – an important factor to consider with young athletes.
- Much of the early management of concussion features reassurance and education.
- What comprises the ‘difficult’ concussion patient?
- Persistent symptoms
- Multiple concussions
- Concussions with diminishing force
- Seizures
- Structural brain injury
- Paediatric injury
- Multiple co-morbidities
- Dix-Hallpike test & Walk-whilst-talk test can be used to assess the potentially concussed athlete – whilst the latter may be used as a management tool http://t.co/ppIEWIeSRJ
Long Term Monitoring of the Retired Athlete Dr Michael Turner
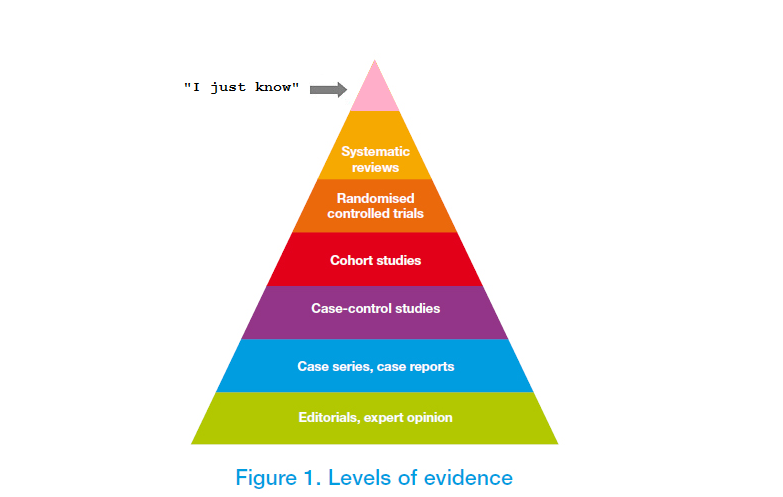
- Consensus statements must be taken with a pinch of salt – evidence constantly evolving and many of the recommendations are based on the ‘I just know’ principle.
- Jockeys are the athletes at greatest risk of developing a concussion. In professional racing a jockey falls off a horse in 1 out of 16 rides, compared to amateur racing where jockeys fall off once every 8 rides. The difference relates to skill level. One jockey dies every 250,000 rides.
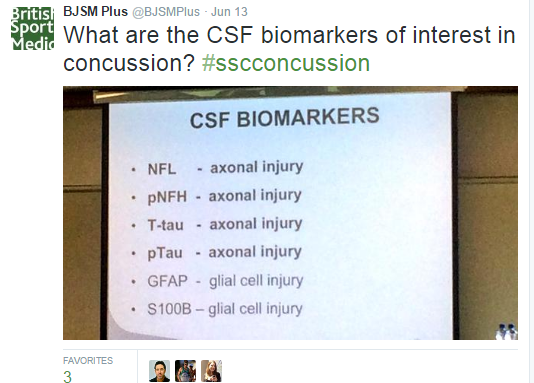
Analysis of CSF Biomarkers in Concussion Dr Sanna Neselius MD, PhD
- Concussions may lead to an increased risk for chronic injuries.
- Several concussions will lead to delayed recovery.
- Neurofilament light (NFL) which although varies with time-of-day may correlate with amount of head trauma.
- NFL may have more of a role to play in delayed recovery than in the initial assessment period.
- Subdural haematoma is the most common sports-related intracranial bleeding.
A Physiological Approach to Assessment and Treatment of Concussion and mTBI Professor Barry Willer PhD
- Return to Play can happen when the athlete can exercise fully without exacerbation of symptoms.
- Issue with return-to-play (RTP) guidelines – return when ‘asymptomatic’ – but when are athletes, let alone controls, fully without symptoms?
- No evidence to support ‘radical rest’, simply academic suggestion – deconditioning may even confer risks to the athlete.
- Role for exercise testing followed by graded exercise protocol (%HRmax) in getting athletes asymptomatic faster, thus potentially accelerating RTP?
- Poor exercise tolerance in the acute phase post concussion may be a marker of poor prognosis.
All papers available at http://t.co/NzRDDn9aKO
***********************************
Dr Sean Carmody is a junior doctor working in the South Thames deanery. He tweets regularly on topics related to sports medicine and performance @seancarmody1.