Fortnightly we invite a colleague to share a clinical tip with our community. Today, Sandro Vella is on the stage.
Who are you?
I am Sandro Vella, a Maltese physiotherapist interested in sports and musculoskeletal physiotherapy. I work as a physiotherapist within the Maltese primary health care system and with the Under/21 Maltese National football team. My passion for sports has fuelled me to further my studies within this field, and after obtaining a Master’s in Sports and Exercise Medicine, I am now reading for a PhD in sports injury prevention. My research focuses on developing, implementing, and evaluating an injury monitoring system for national team football players.

What clinical tips would you like to share with the community?
One of the main challenges clinicians face is the lack of athlete adherence to the recommended rehabilitation plans. The reasons for non-adherence are complex and involve an interaction between athletes, clinicians, and the broader social environment. As a result, rehabilitation outcomes may not always be successful.
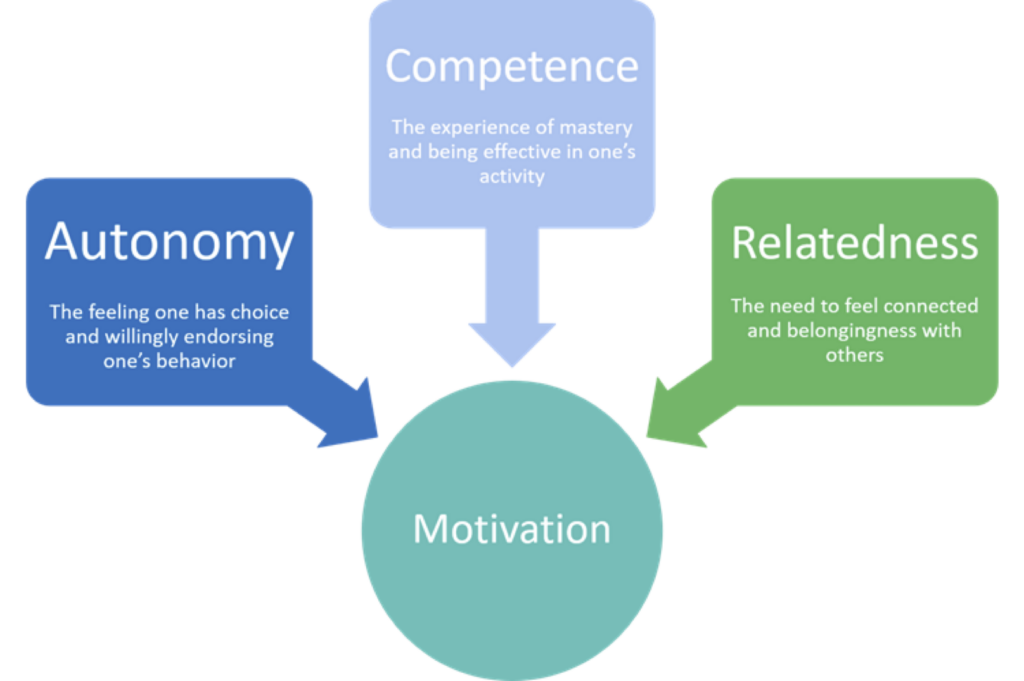
In enhancing adherence, the Self-Determination Theory (SDT) can provide useful insights. SDT posits that humans become self-determined and autonomously motivated to carry out a task when their basic psychological needs are fulfilled. Specifically, this requires autonomy, competence, and relatedness (Figure 1).
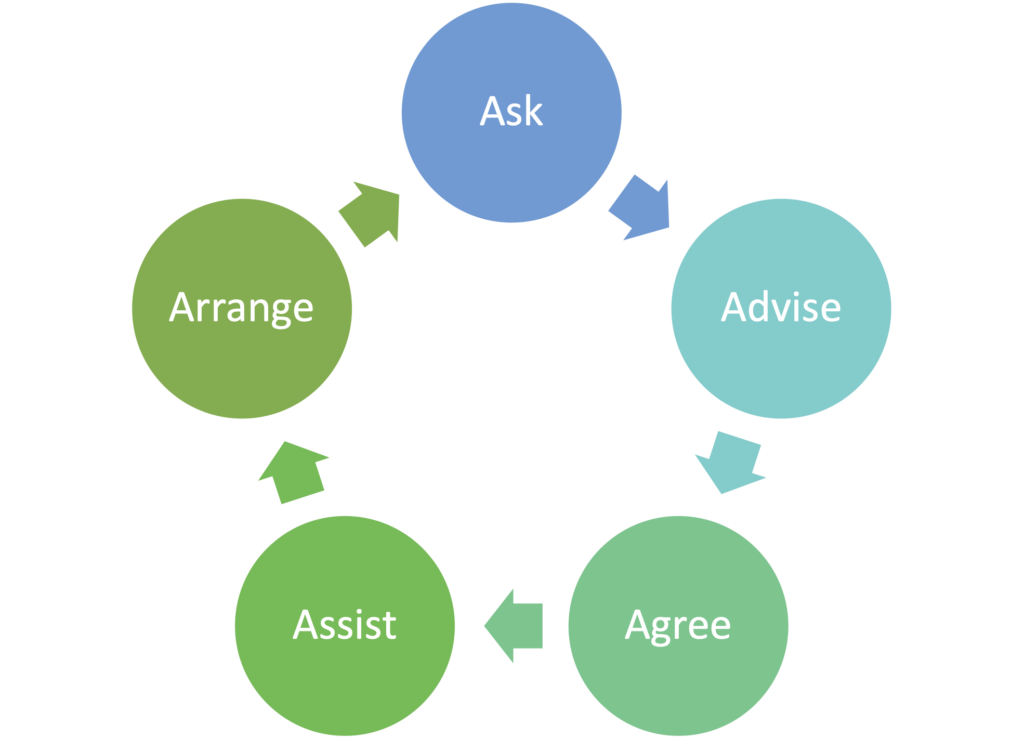
Theoretically, meeting the three basic psychological needs would improve athlete adherence to rehabilitation programmes. Practically, communicating effectively in a caring and autonomy-supportive way can enhance adherence. This is where the 5 A’s framework (Figure 2) provides an effective way to translate the three psychological tenets into practice. Each ‘A’ from the 5 ‘A’s includes communication strategies that can be used in conversation with athletes to motivate them to adhere to the recommended rehabilitation plan.
I have provided some strategies and examples of how to incorporate such communication strategies within each ‘A’:
| Strategy | Example |
| ASK | |
| Use single open-ended questions. | ‘Can you tell me about your problem?’ |
| Stay silent while listening to their problem, then summarise and empathise. | ‘What I am hearing is… This must feel frustrating for you.’ |
| Gauge readiness to accept advice. | ‘I understand your problem… would you like to hear some suggestions to overcome this problem?’ |
| ADVISE | |
| Individualise educational methods (e.g. visual and verbal) for each athlete, making sure to meet their preferences. | |
| Close the loop and provide corrective feedback. | ‘To make sure that you understood, could you summarise what you understood from this information?’ |
| Provide opportunities for athlete input. | ‘Some types of exercise can help you increase your fitness levels while recovering from a hamstring injury, for example, riding a bike and swimming. Which exercise type do you prefer at this stage?’ |
| Provide a rationale for exercise choices while providing autonomous supportive phrases. | ‘Your hamstrings need strength work. Working on the agreed exercises can increase your hamstring strength and reduce your likelihood of re-injury.’ |
| AGREE | |
| Employ SMART (specific, measurable, accurate, realistic, and timely) goals. | ‘For the next week, could we set the goal of doing 12 repetitions for three sets?’ Can you incorporate this exercise plan once every alternate day in the coming week?’ |
| Ensure active participation during goal setting. | ‘What time of day would suit you best to carry out the exercise programme?’ |
| ASSIST | |
| Identify barriers. | ‘What likely obstacles may prevent you from accomplishing this goal?’ |
| Identify solutions to the barriers. | Instead of allowing the injured athlete to feel demotivated to perform the exercises alone, you could ask, for example: ‘How would you feel performing the exercise program in the gym while in the company of your teammates?’ |
| ARRANGE | |
| Ask the athlete to keep track of their rehabilitation process by recording and tracking their accomplished goals in a rehabilitation diary or an exercise tracker on a mobile application. | |
| Follow-up. | ‘We can meet in one week to re-assess strength and modify the exercise plan accordingly.’ |
| Offer contact. | ‘Please contact me whenever you want to clear something out.’ |
Table 1: Mapping communication strategies to the ‘5A’ framework
Where does it come from?
Through my experience as a clinician, I have realised that simply providing athletes with a rehabilitation plan does not always translate to intended results, with non-adherence playing a large role. This begged the questions: How could I enhance athlete adherence to injury rehabilitation plans? This question played a major role in the design of my PhD studies, in which one of my main objectives was to understand how athletes perceive an injury and how this informs its management. Answering such a question by listening to the athletes’ perspectives allowed me to understand better how I could improve my clinical and communication skills to enhance athlete adherence to the recommended injury rehabilitation plans.
What is its scientific evidence, if any?
The clinical tip related to the three basic psychological needs and 5 A’s framework is evidence-based. The SDT1 is a theory widely utilised in different research areas to understand human behaviour. The 5 A’s framework, based on fulfilling the SDT psychological tenets, was initially developed to support tobacco users during the process of smoking cessation. Unfortunately, there is limited research using this framework within other health domains2. Therefore, I acknowledge that although the framework is helpful for clinical practice, more research is required to align the 5 A strategies to athletes.
References
- Johan et al., (2012). Self-determination theory applied to health contexts: A meta-analysis. Perspectives on Psychological Science 7(4): 325 – 340.
- Lonsdale et al. (2012). Communication style and exercise compliance in physiotherapy (CONNECT). A cluster randomized controlled trial to test a theory-based intervention to increase chronic low back pain patients’ adherence to physiotherapists’ recommendations: Study rationale, design, and methods. BMC Musculoskeletal Disorders 13(1): 104.