Lower extremity injury rates in sport are high and have significant consequences; however, the current evidence to inform the prevention of lower extremity injuries female/woman/girl athletes is sparse. Our team recently conducted a systematic review and meta-analysis to assess the effectiveness of female/woman/girl athletes’ lower-extremity injury prevention strategies [e.g., training strategies, personal protective equipment (PPE), policy/rules, and injury management] and their unintended consequences.
Why is this important?
Lower-extremity injuries account for over 60% of all female/woman/girl sport injurie (1, 2). In any given season, up to 50% of female/woman/girl athletes playing a variety of sports will experience a lower-extremity injury (2, 3). These injuries have a high financial cost (4-6) and short and long-term consequences (7-11). However, the majority of the current evidence is derived from male/man/boy athletes, or data combining genders/sexes with few studies considering female/women/girl-specific data.
Lower-extremity injury prevention interventions include neuromuscular training-based injury prevention programs (NMT) that include balance, strength, agility, and/or running/movement/cutting drills, personal protective equipment (PPE), policy/rule changes, and injury management (12-16). While some information is known concerning the efficacy of NMT programs (17-19), these data are inconsistent. There is currently little-known concerning PPE, policy/rule changes, or injury management. The absence of detailed information has limited clinical interpretation and application of injury-prevention strategies in female/woman/girl sports. Analyzing existing female/women/girl-specific data could enhance the understanding of the effectiveness of lower-extremity injury prevention strategies for female/woman/girl athletes and enable sport partners—such as athletes, coaches, clinicians, parents, and community sport organizations—to implement evidence-informed best practices and policies for injury prevention.
How did we study this?
We reviewed and included 82 studies and performed a meta-analysis on studies that specifically reported the effects of female/woman/girl NMT training on lower extremity injury. Of note, 7% of all studies did not report the number or % of sex or gender when female/woman/girl and male/man/boy athletes were included. There was not sufficient data to perform meta-analysis for PPE, policy/rules, or injury management.
What did the study find?
Across the 82 studies, a total of 154,561 participants (84,915 females/women/girls, 55%) were included. Neuromuscular-based training programs [(NMT) n=60, 73%] were the most frequently studied prevention strategy, followed by personal protective equipment (PPE) (n=9, 11%), policy/rules change (n=4, 5%), and 6 (7%) education. Of note, 7% of all studies did not report the number or % of sex or gender when female/woman/girl and male/man/boy athletes were included. There was not sufficient data to perform meta-analysis for PPE, policy/rules, or injury management.
- There was low certainty of evidence from 9 studies that NMT training programs with a minimum dose of 10 minutes twice weekly, reduced female/woman/girl athletes’ lower extremity injuries by 19%
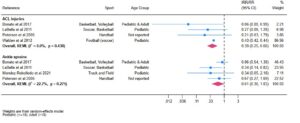
- There was moderate certainty of evidence from 6 studies that NMT training programs reduce ankle sprains by 39%.
- There was high certainty of evidence from 6 studies that NMT training programs reduce anterior cruciate ligament injuries by 61% (Figure 1).
Figure 1
What are the key takeaways?
- Neuromuscular training programs that include at least 10 minutes of exercise twice per week, progressing from bilateral to single-leg activities and incorporating balance, lower-limb strength, agility, and directional changes, are effective in reducing ankle sprains and anterior cruciate ligament (ACL) injuries among female/woman/girl athletes of all ages.
- Due to the relatively low resource demands of neuromuscular injury-prevention programs, there is significant potential for national and international policy initiatives to mandate their widespread adoption in female/woman/girl athlete sports.
- Current evidence is limited regarding strategies to prevent lower-extremity injuries in female/woman/girl athletes beyond the knee and ankle, as well as the effectiveness of interventions such as rule modifications, protective equipment, or educational approaches.
Authors:
Garrett S. Bullock [1,2]
Jackie L. Whittaker [2,3]
Maitland Martin [2]
Chelsea L. Martin [4]
Carolyn A. Emery [2]
Affiliations
- Department of Orthopaedic Surgery & Rehabilitation, Wake Forest University School of Medicine, Winston-Salem, North Carolina, USA
- Sport Injury Prevention Research Centre, Faculty of Kinesiology, University of Calgary, Calgary, Alberta, Canada.
- Department of Physical Therapy, University of British Columbia, Vancouver, Canada
- Department of Epidemiology, Gillings School of Global Public Health, University of North Carolina at Chapel Hill, North Carolina, USA
References
- Emery CA, Meeuwisse WH, McAllister JR. Survey of sport participation and sport injury in Calgary and area high schools. Clinical journal of sport medicine 2006;16(1):20-26.
- Roos KG, Marshall SW, Kerr ZY, et al. Epidemiology of overuse injuries in collegiate and high school athletics in the United States. The American journal of sports medicine 2015;43(7):1790-97.
- Richardson A, Clarsen B, Verhagen E, Stubbe JH. High prevalence of self-reported injuries and illnesses in talented female athletes. BMJ open sport & exercise medicine 2017;3(1):e000199.
- Tenan MS. Quantifying emergency department visits from sport and recreation: focus on the lower extremity and knee, 1997–2009. Journal of Athletic Training 2016;51(4):309-16.
- King D, Hume PA, Hardaker N, et al. Sports-related injuries in New Zealand: National Insurance (Accident Compensation Corporation) claims for five sporting codes from 2012 to 2016. British journal of sports medicine 2019;53(16):1026-33.
- Ross AG, McKay MJ, Pappas E, et al. Direct and indirect costs associated with injury in sub-elite football in Australia: a population study using 3 years of sport insurance records. Journal of science and medicine in sport 2022;25(9):743-49.
- Richmond SA, Fukuchi RK, Ezzat A, et al. Are joint injury, sport activity, physical activity, obesity, or occupational activities predictors for osteoarthritis? A systematic review. journal of orthopaedic & sports physical therapy 2013;43(8):515-B19.
- Whittaker JL, Woodhouse L, Nettel-Aguirre A, Emery C. Outcomes associated with early post-traumatic osteoarthritis and other negative health consequences 3–10 years following knee joint injury in youth sport. Osteoarthritis and cartilage 2015;23(7):1122-29.
- Ezzat AM, Brussoni M, Mâsse LC, Emery CA. Effect of anterior cruciate ligament rupture on physical activity, sports participation, patient-reported health outcomes, and physical function in young female athletes. The American journal of sports medicine 2021;49(6):1460-69.
- Filbay SR, Skou ST, Bullock GS, et al. Long-term quality of life, work limitation, physical activity, economic cost and disease burden following ACL and meniscal injury: a systematic review and meta-analysis for the OPTIKNEE consensus. British Journal of Sports Medicine 2022;56(24):1465-74.
- Bruder AM, Culvenor AG, King MG, et al. Let’s talk about sex (and gender) after ACL injury: a systematic review and meta-analysis of self-reported activity and knee-related outcomes. British journal of sports medicine 2023;57(10):602-10.
- Emery CA, Roy T-O, Whittaker JL, et al. Neuromuscular training injury prevention strategies in youth sport: a systematic review and meta-analysis. British journal of sports medicine 2015;49(13):865-70.
- Herman K, Barton C, Malliaras P, Morrissey D. The effectiveness of neuromuscular warm-up strategies, that require no additional equipment, for preventing lower limb injuries during sports participation: a systematic review. BMC medicine 2012;10:1-12.
- Lauersen JB, Bertelsen DM, Andersen LB. The effectiveness of exercise interventions to prevent sports injuries: a systematic review and meta-analysis of randomised controlled trials. British journal of sports medicine 2014;48(11):871-77.
- Yang J, Marshall SW, Bowling JM, et al. Use of discretionary protective equipment and rate of lower extremity injury in high school athletes. American journal of epidemiology 2005;161(6):511-19.
- McBain K, Shrier I, Shultz R, et al. Prevention of sport injury II: a systematic review of clinical science research. British journal of sports medicine 2012;46(3):174-79.
- Crossley KM, Patterson BE, Culvenor AG, et al. Making football safer for women: a systematic review and meta-analysis of injury prevention programmes in 11 773 female football (soccer) players. British journal of sports medicine 2020;54(18):1089-98.
- Emery CA, van Den Berg C, Richmond SA, et al. Implementing a junior high school-based programme to reduce sports injuries through neuromuscular training (iSPRINT): a cluster randomised controlled trial (RCT). British journal of sports medicine 2020;54(15):913-19.
- Slauterbeck JR, Choquette R, Tourville TW, et al. Implementation of the FIFA 11+ injury prevention program by high school athletic teams did not reduce lower extremity injuries: a cluster randomized controlled trial. The American Journal of Sports Medicine 2019;47(12):2844-52.