Part of the BJSM’s #KnowledgeTranslation blog series
In this blog, we will explain how the results of a very simple, rapid, safe and objetive test to assess static balance could be clinically useful. Our study (recently published in BJSM) was conducted by a group of investigators from different countries of the world – Brazil, UK, USA, Finland and Australia – that jointly analyzed data from the CLINIMEX Exercise cohort (Rio de Janeiro, Brasil) obtained between 2008 to 2020.
Why is this study important?
All human beings should aim to be physically fit. For older individuals, beyond aerobic fitness, it is likely that other non-aerobic components of physical fitness – such as muscle power and balance- would also be relevant to their health. In this regard, balance has been reported to be quite stable until the fifties, after which it quickly diminishes, impairing autonomy and increasing the risk for falls and other adverse health outcomes. Unfortunately, despite its widely recognized relevance, balance is not routinely evaluated in most clinical settings in older individuals. This may be partly attributable to the poor standardization of balance testing as well as to the relative paucity of data relating balance results to clinical outcomes other than falls, such as mortality, when compared to, for example, aerobic fitness.
How did the study go about this?
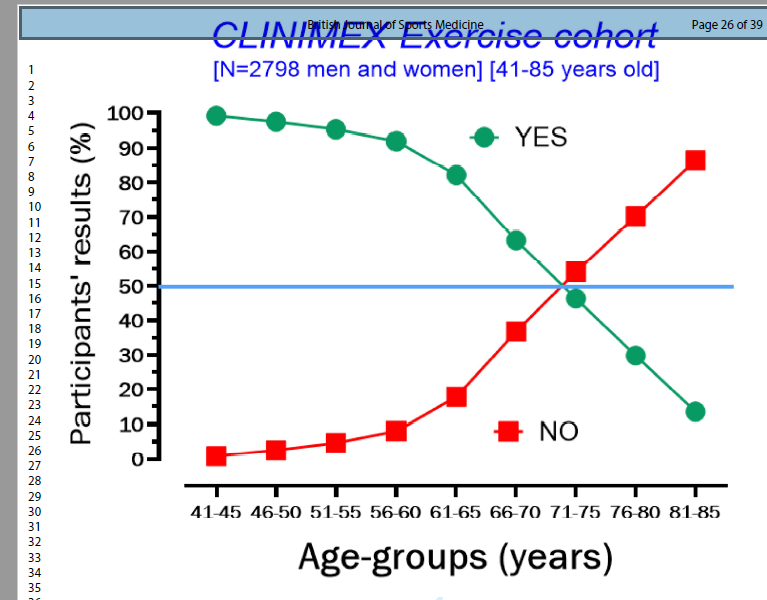
The CLINIMEX Exercise open cohort (Rio de Janeiro, Brazil) includes data from all evaluations undertaken since 1994, including several demographic, clinical and physiological variables as well as periodic checking of individual’s vital status. Starting in 2008, balance assessment has been incorporated in this evaluation protocol. In particular, a 10-second one-legged stance (10s OLS) test was conducted using right and left leg, with the results being expressed according to ability (YES) or inability (NO) to complete the 10s OLS test.
What did the study find?
We have analysed the data aiming to identify the age pattern of YES and NO responses to 10s OLS and to assess whether is any the relationship between this response and all-cause mortality. Initially selecting individuals older than 40 years of age, as expected, we confirmed that the inability to complete the 10s OLS increases with aging and that a 50/50 YES-NO pattern of response occurred around 70 years of age. In other words, for individuals younger than 75 years of age the most common response to the 10s OLS is YES, while for those older, the opposite occurs (see figure 1).
Further analyzing our 10s OLS results at 5-year of age intervals, we found that the 10s OLS was able to better discriminate static balance responses between 51 and 75 years of age. This allow us to, in sequence, proceed to answer a very relevant question in public health: does a successful 10s OLS performance predict survival in older adults? The response is yes!
By analyzing 10s OLS data from 1702 individuals who were fully ambulatory and not exhibiting unstable gait or signs of acute vestibular or otoneurological disturbances in the evaluation (68% men), in combination with several other variables, and having access to survival data – median follow-up of 7 years and 7.2% of individuals died -, we found that the proportion of deaths was 3.8 times higher among the NO responders as compared with YES responders to 10s OLS; 17.5% and 4.6%, respectively. The calculated hazard ratio for all-cause mortality was 1.84 [95% CI:1.23-2.78] (P<0.001) for the individuals unable to complete 10s OLS as compared with those that successfully completed this task, when adjusted for age, sex, body mass índex and several comorbities.
What are the key take-home points?
The advantages of the 10s OLS test include that it is simple and it provides rapid, safe and objective feedback for the patient and health care providers regarding static balance. Thus, it can be easily incorporated into the routine of the most clinical consultations, especially for older adults. Importantly, the 10s OLS results add useful information regarding mortality risk in middle-aged and older men and women beyond ordinary clinical data.
Author and Affiliations:
Claudio Gil S Araújo, MD, PhD1; Christina Grüne de Souza e Silva, MD, PhD1; Jari Antero Laukkanen, MD, PhD2,3; Maria A Fiatarone Singh, MD4; Setor K Kunutsor, MD, PhD5,6; Jonathan Myers, PhD7; João Felipe Franca, MD1; Claudia Lucia Castro, MD, MSc1
- Exercise Medicine Clinic – CLINIMEX – Rio de Janeiro, Brazil.
- Institute of Clinical Medicine, Department of Medicine, University of Eastern Finland, Kuopio, Finland.
- Central Finland Health Care District, Department of Medicine – Jyväskylä, Finland.
- School of Health Sciences and Sydney Medical School, Faculty of Medicine and Health, University of Sydney, Sydney, Australia.
- National Institute for Health Research Bristol Biomedical Research Centre, University Hospitals Bristol and Weston NHS Foundation Trust and the University of Bristol – Bristol, UK.
- Translational Health Sciences, Bristol Medical School, University of Bristol, Learning & Research Building (Level 1), Southmead Hospital – Bristol, UK.
- VA Palo Alto Health Care System and Stanford University – United States – Palo Alto, US.
Claudio Gil Araújo, MD, PhD (cgaraujo@iis.com.br)