By Dr Nicky Keay @nickyKfitness
Now is a good time to revisit a topic discussed in my previous BJSM blog([i]), to coincide with guidelines on the management of thyroid disease released by National Institute of Clinical Excellence (NICE) in November 2019([ii]), and summarised in the British Medical Journal (BMJ) last month([iii]).
It has transpired that athletics coach Alberto Salazar facilitated the clinically inappropriate prescription of thyroxine to some of his euthyroid athletes. Thyroxine is not on the World Anti-Doping Agency’s (WADA) banned list, nevertheless as we shall discuss below, administering thyroxine to those with normal thyroid function potentially can have adverse consequences on health and performance. Salazar was banned for four years on the grounds outlined by United States Anti Doping Agency (USADA) ([iv]), falling into three areas: use of a prohibited method (with infusion in excess of the limit), tampering with the doping control process, and trafficking of testosterone.
Recap of thyroid axis
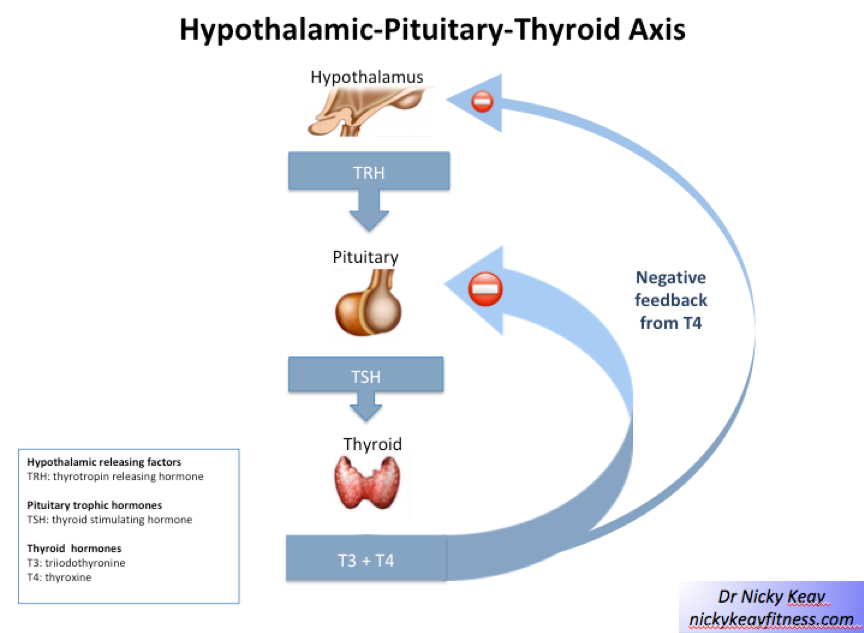
In common with many endocrine axes, the thyroid axis works on a negative feedback loop mechanism to maintain homeostasis of circulating levels of the response hormone thyroxine (T4) in the normal range. TSH (thyroid stimulating hormone) is the control hormone released by the pituitary gland. TSH acts on the thyroid gland to release T4, which in turn is converted peripherally to the more active T3. As with all biological homeostatic mechanisms, there is some physiological variation within the normal range for an individual. Significant changes, beyond that expected from biological and analytical variation can be calculated using the system recently described in BMJ ([v]).
Significant patterns in thyroid function
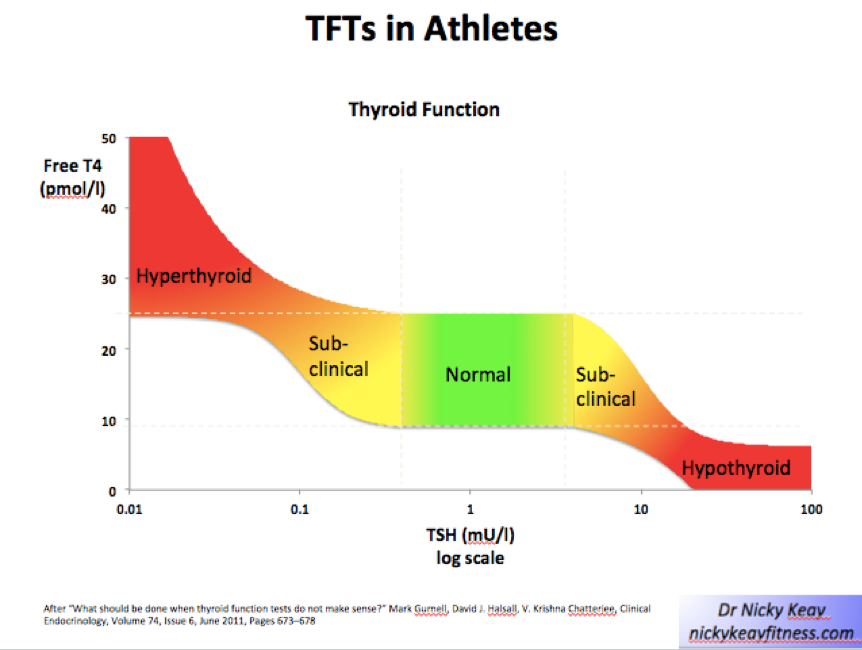
Consecutively raised TSH levels, with paired levels of T4 below the normal range indicate primary hypothyroidism.
Conversely, levels of TSH below the normal range with paired levels of T4 above the upper end of the normal range indicate an overactive thyroid.
If the situation were that clear-cut, then this would be a very short blog. Needless to say, there are some situations requiring careful scrutiny.
Subclinical hypothyroidism is the situation where TSH is raised above the upper end of the normal range, yet T4 remains in range. According to NICE guidelines thyroxine treatment is indicated where TSH >10 mlU/L on 2 occasions, 3 months apart OR in someone under 65 years of age, where TSH is raised above the reference range (but lower than 10 mlU/L) on 2 occasions, 3 months apart AND accompanied by symptoms of hypothyroidism. Furthermore, NICE advises that any treatment with thyroxine should be such that TSH is maintained in the normal range and NOT cause suppression of TSH, nor symptoms of thyrotoxicosis.
Based on this clinical criteria, some athletes under Salazar were reportedly treated inappropriately with thyroxine. In other words, even when TSH was in the normal range and the athletes were in euthyroid status, in the absence of an indication of subclinical hypothyroidism, it appears that thyroxine was given in the belief that this might aid with maintaining low body weight, which could be a performance advantage. Nevertheless, WADA does not consider thyroxine to confer a performance advantage, which is why this hormone is not on the banned list.
However, treatment with thyroxine, which is not warranted on clinical grounds, can potentially have adverse effects on health, for example, increased risk of cardiac arrhythmias. Moreover, it is well documented that thyrotoxicosis is a risk factor for bone fracture in the long term. In the short term, stress fractures in athletes are recognised as a consequence of low energy availability[vi], which is the underlying aetiology of relative energy deficiency in sport (RED-S)([vii]). Increased metabolic rate as a consequence of endogenous or exogenous excess thyroxine could theoretically lead to a situation of unintentional low energy availability and the adverse clinical sequalae of RED-S.
“Non thyroidal illness”/ “sick euthyroid” is characterised by low-end range TSH and T4. In other words, the negative feedback loop to maintain hormone homeostasis is not functionally normally. This situation is seen in functional hypothalamic-pituitary-endocrine gland suppression: for example, in athletes and dancers with the clinical syndrome of RED-S. In female athletes RED-S often presents as functional hypothalamic amenorrhoea, with low FSH and LH (in the presence of normal prolactin) and low oestrogen. As part of the adaptive response to the situation of low energy availability, metabolic rate is down-regulated to “save energy” ([viii]) characterised by low-end range TSH, T4 and T3 ([ix]). In such a situation, giving exogenous thyroxine will override this physiological response to down regulate metabolic rate and potentially increase energy deficit.
The psychological and physical pressures experienced by athletes and dancers can sometimes have reversible impacts on the hypothalamic-pitutary-thyroid axis. On the other hand, athletes and dancers can also experience medical conditions, which impact this endocrine axis. The recognition of these different situations provides insights and a deeper understanding of overall endocrine function in this athletic population.
***
References
[i] Keay N. Fatigue, sport performance and hormones….more on the endocrine system. Posted on May 25, 2017 by BJSM
[ii] Thyroid disease: assessment and management NICE guideline [NG145]. Published date: November 2019
[iii] Thyroid disease assessment and management: summary of NICE guidance
BMJ 2020; 368 doi: https://doi.org/10.1136/bmj.m41 (Published 29 January 2020) Cite this as: BMJ 2020;368:m41
[iv] AAA Panel Imposes 4-Year Sanctions on Alberto Salazar and Dr. Jeffrey Brown for Multiple Anti-Doping Rule Violations September 2019 USAD
[v] Your results may vary: the imprecision of medical measurementsBMJ 2020; 368 doi: https://doi.org/10.1136/bmj.m149 (Published 20 February 2020) Cite this as: BMJ 2020;368:m149
[vi] Heikura I, Uusitalo A, Stellingwerff T et al Low Energy Availability Is Difficult to Assess but Outcomes Have Large Impact on Bone Injury Rates in Elite Distance Athletes. International Journal of Sport Nutrition and Exercise Metabolism2018; 28 (4), 403-11
[vii] Keay N. 2018 UPDATE: Relative Energy Deficiency in Sport (RED-S). Posted on May 30, 2018 by BJSM
[viii] Staal S, Sjödin A, Fahrenholtz I Low RMR ratio as a Surrogate Marker for Energy Deficiency, the Choice of Predictive Equation Vital for Correctly Identifying Male and Female Ballet Dancers at Risk International Journal of Sport Nutrition and Exercise Metabolism 2018
[ix] Ihle R, Loucks A Dose-response relationships between energy availability and bone turnover in young exercising women Journal of Bone and Mineral Research (2004) 19(8) 1231-1240