Fortnightly we invite a colleague to share a clinical tip with our community. Today, Ana Azevedo is on the stage.
Who are you?
I am Ana Morais Azevedo, musculoskeletal and sports physiotherapist. I hold a postgraduate sport physiotherapy degree and a PhD on dancers’ lower extremity landing biomechanics. My clinical work, curiosity, and interest of the foot-ankle complex led me to travel more than 17.000 km to expand my knowledge and skills. Thus, I am currently Down Underwhere I started a 2nd PhD on foot morphology, strength and performance in dancers, runners, and the general population.

What clinical tip would you like to share with the community?
Single-leg heel raises (SLHR) are a valuable clinical test that can provide more clinical information than just strength and endurance capacity. It can also be useful as a screening tool for the foot-ankle complex, in particular the foot muscles. The intrinsic (origin and insertion within the foot) and extrinsic (origin outside the foot and insertion within the foot) foot muscles work together in functional groups in many lower extremity activities, including the SLHR.
While performing barefoot weightbearing SLHR, observe the general quality of movement (Table 1.A.) as well as counting the number of repetitions. But it is also important to look at the distal part (Table 1.B.), such as the foot-ankle complex quality of movement (i.e., behaviour/pattern of the toes). What to look at? A checklist of important details (Table 1.) should be considered throughout the repetitions of the SLHR. Also see this video.
Table 1. Checklist for single-leg heel raises.
| A. | Y/N | Comments |
| Is the lower extremity aligned (knee, leg, ankle, foot)? | ||
| Is the knee in a neutral position (not flexed or hyperextended)? | ||
| Is the person keeping the same pace? | ||
| Is the full range of motion free of pain? | ||
| Is the movement being stopped just before feeling pain? | ||
| Is every repetition performed at the maximal height of ankle plantar flexion? | ||
| Does the movement have a smaller amplitude as the test progresses? If so, at which repetition does the height diminish? | ||
| Is the movement smooth and controlled rather than sharp or irregular? | ||
| Is the body moving vertically rather than rocking forward? | ||
| B. | Y/N | Comments |
| Is the foot in a parallel position? | ||
| Is the middle of the ankle aligned with the 2nd metatarsal (not fishing or sickling the foot)? | ||
| What are the toe movement patterns during the repetitions? | ||
| o Are the toes long and flat? | ||
| o Are the toes and metatarsal heads always keeping contact with the floor? | ||
| o Are the toes curling (i.e., claw, hammer, mallet toes)? | ||
| o Do the toes curl at the start of the test? | ||
| o Do the toes curl during the test? On which repetition do they curl? | ||
| o Is dynamic valgus of the hallux present? | ||
| o Is the weight distributed between the 1st and 5th toes? | ||
Why does dynamic deformity (toe curling) occur while performing SLHR? Toe curling (i.e., claw, hammer, mallet toes) presents as flexion and/or extension of the interphalangeal and/or metatarsophalangeal joints (Figure 1). If the person cannot keep the neutral position of the interphalangeal and metatarsophalangeal joints, by maintaining contact of the toes and metatarsal heads against the floor, this may be a clinical sign of a deficit in the strength of the intrinsic foot muscles and overactivity of the extrinsic muscles such as flexor digitorum longus and flexor hallucis longus. This might be due to an imbalance between the activation of the extrinsic and intrinsic foot muscles and may lead to lower extremity overuse injuries (i.e., flexor hallucis longus tenosynovitis). These toe deformities during SLHR may also be associated with a lack of strength-endurance of the gastrocnemius. As the person repeats the SLHR endurance test, the flexor hallucis longus and flexor digitorum longus may compensate for a gastrocnemius with poor endurance. Toe curling at the height of the SLHR or as the test progresses can be a sign of gastrocnemius fatigue and overactivity of the long toe flexors.
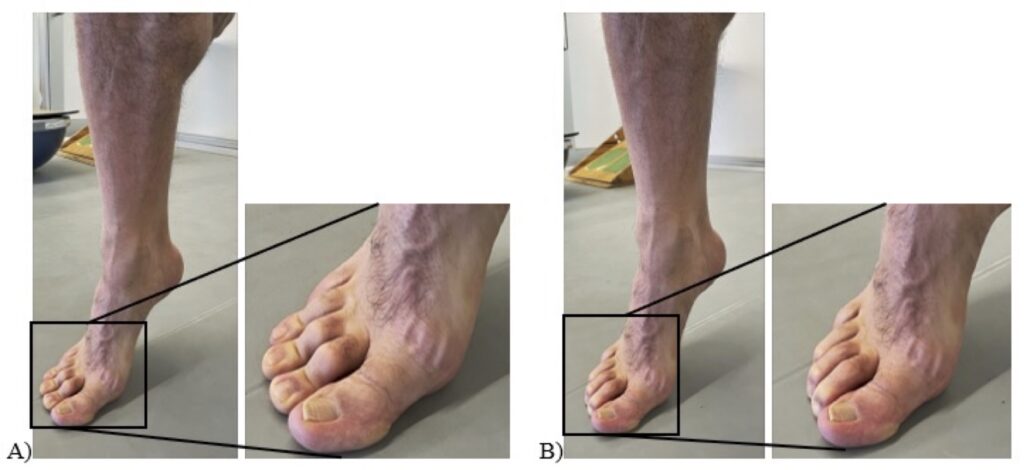
Figure 1. Toe curling: A) Hammer toes and B) Claw toes during single-leg heel raises (Dancer: Sakis Michelis)
The SLHR can be performed in any clinical setting or sports facility. No equipment is required; it just needs a place to lightly put the fingertips to assist with balance. It can also be an assessment test and an exercise in rehabilitation or intervention programs. The test also provides feedback about progression and improvement (i.e., number of repetitions, height of the heel, foot-ankle alignment, toes movement pattern, compensatory movements, extension range of toes, metronome pacing, etc.). Normative data related to the number of repetitions can be found here.3 On a side note, the use of a metronome is a helpful tool to keep pace (adjusted to each person and technique) avoiding speeding up or slowing down during the SLHR. Variations to the speed over time are important and can be manipulated accurately with a metronome.
Where does it come from?
The foot is the interface between the lower extremity and the ground and is often overlooked in lower extremity injury management programs and rehabilitation. However, we rely on this intricate structure in our daily and sports activities.
Over time I have noticed in my clinical practice, and then in my PhD, how the biomechanics of the foot is critical to the lower extremity kinetic chain and its functionality. Additionally, recent literature has been highlighting the importance of the foot, particularly the intrinsic foot muscles and its association to foot pain, function, and performance. Physiotherapist Sue Mayes, Director of Artistic Health at The Australian Ballet and fellow researcher at La Trobe University, has been developing a great clinical body of work related to the foot-ankle complex in athletic populations (i.e., dancers and football players). The SLHR has been an important test and exercise used at The Australian Ballet for over 20 years. Improved calf and foot capacity is thought to have led to a very low incidence of foot and ankle injury, and surgery is rarely required at The Australian Ballet. Sue has been highlighting the importance of assessing and treating the foot-ankle complex due to the high daily demands of load and intensity and its potential impact on the lower extremity injuries in dance and sport.
What is its scientific evidence, if any?
This clinical tip related to the foot muscles is evidence-based (see references below) and based on clinical reasoning and clinical experience. It might be an approach with practical implications for evaluation of foot muscle dynamic deficits.
Despite the challenging constraints to study the intrinsic foot muscles due to anatomical configuration, location and potential overlapping functions between intrinsic and extrinsic foot muscles,6,9 it is known that the intrinsic foot muscles have a role to dissipate and generate mechanical energy, providing versatility of human foot function.8,1,5
More attention should be given to the foot muscles in clinical practice. The intrinsic foot muscle activity increases in response to postural demands.6,2,4 The intrinsic and extrinsic foot muscles work together as a functional group in double-leg and single-leg postures. The intrinsic foot muscles are significantly activated in double and single-leg heel raises, with higher muscular activity in single-leg positions than double-leg,6 therefore the magnitude of loading and the type of movement matter for foot muscles. The intrinsic foot muscles should be highly loaded during lower extremity exercises to provide balanced activation between intrinsic and extrinsic foot muscles. Further understanding of the foot muscles function during high-load activities in athletic and non-athletic populations is needed. Stay tuned!
References
- Farris et al. (2019). The functional importance of human foot muscles for bipedal locomotion. PNAS, 116, 5:1645-1650.
- Ferrari et al. (2020). Intrinsic foot muscles act to stabilise the foot when greater fluctuations in the centre of pressure movement result from increased postural balance challenge. Gait & Posture, 79: 229-233.
- Hebert-Losier et al. (2017). Updated reliability and normative values for the standing heel-rise test in healthy adults. Physiotherapy, 103: 446-452.
- Kelly et al. (2012). Recruitment of the plantar intrinsic foot muscles with increasing postural demand. Clin Biomech, 27: 46-51.
- Kelly et al. (2019). Intrinsic foot muscles contribute to elastic energy storage and return in the human foot. J Appl Physiol, 126: 231-238.
- Ridge et al. (2022). Contributions of Intrinsic and Extrinsic Foot Muscles during Functional Standing Postures. Biomed Res Int, Article ID 7708077.
- Sauer et al. (2011). Considering the Intrinsic Foot Musculature in Evaluation and Rehabilitation for Lower Extremity Injuries. Athl Train & Sport Health Care, 3(1): 43-47.
- Smith et al. (2022). Flexor digitorum brevis utilises elastic strain energy to contribute to both work generation and energy absorption at the foot. J Exp Biol, 225(8).
- Soysa et al. (2012). Importance and challenges of measuring intrinsic foot muscle strength. J Foot and Ankle Res, 5:29.