One reason why the covid-19 pandemic is predicted to last until at least 2028 is that rich countries are hoarding vaccines, leaving very few doses for low- and middle-income countries (LMICs). Many rich nations have blocked LMICs from making their own doses, so global vaccine distribution must rely on a “trickle down” charity model in which the rich world donates doses to LMICs––a “crumbs from the rich person’s table” approach. But the charity model has been a catastrophic failure.
For example, Canada and Libya have roughly the same covid-19 incidence rate (cumulative covid-19 cases per million population) at time of writing, but have starkly different access to vaccines. As of 17 August 2021, 73% of Canada’s population has had at least one dose compared with just 11% in Libya. Germany and Botswana have a similar incidence rate as well, but in Germany, 55% of people are fully vaccinated, while in Botswana only 5.6% are.
Which nations are the biggest hoarders? Since November 2020, Duke University has been tracking every country’s vaccine purchases and comparing the number of purchased doses with the population of each nation. Right now, the gold medal for top hoarder goes to Canada, which has purchased enough shots to vaccinate its entire population 5.2 times over. Australia wins silver, with enough doses to vaccinate its population 4.6 times. The United Kingdom wins bronze by procuring sufficient doses to vaccinate every citizen at least 4 times over. The EU is not far behind, with enough doses to vaccinate everyone 3.5 times over.
There is an irony in the fact that many of today’s biggest hoarders were nations that mounted terrible responses to the pandemic, particularly in the first year. There have been multiple in-depth reports of the mishandling of covid-19 by the governments of Canada, the UK, and Europe. Having bungled their initial pandemic management—for example, poor execution of test-and-trace interventions or acting too slowly in instituting stay-at-home orders and adopting community-wide masking—they are now arguably trying to over-compensate by purchasing way more vaccine doses than they need.
Another thing is very striking about the hoarders: on the Global Health Security Index (GHSI), which ranks 195 countries based on a set of “global health security capabilities,” they tend to have higher scores. In other words, nations that are ranked as “best prepared” on this index are also more likely to be covid-19 vaccine hoarders.
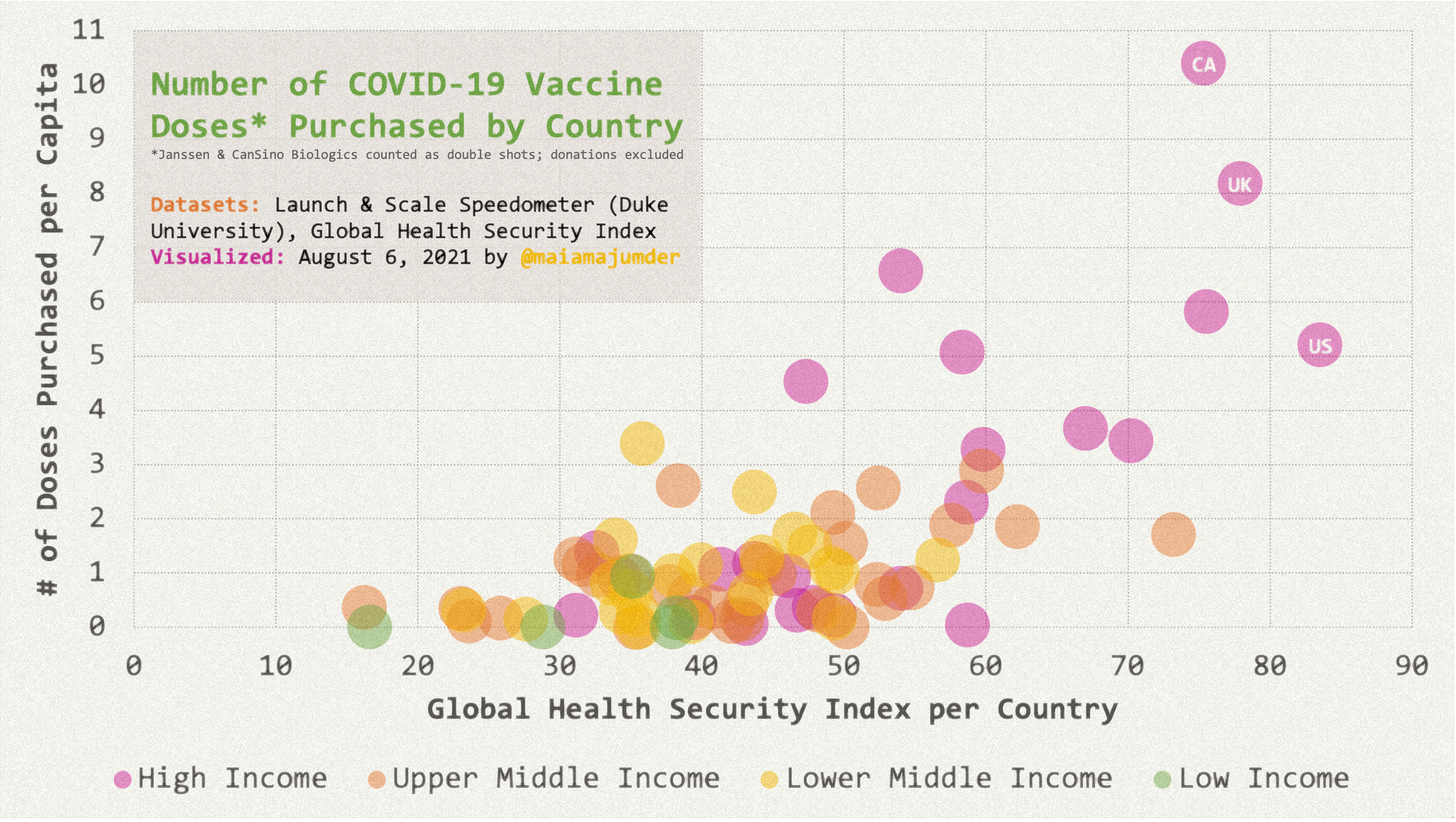{kind=link}
Each nation is given a score on the index between 0 (worst prepared) and 100 (best prepared). The scoring is based on an external assessment of a nation based on its capabilities across six categories: (i) preventing the emergence of pathogens; (ii) detecting and reporting outbreaks; (iii) rapid outbreak response; (iv) health system strengthening; (v) compliance with international norms; and (vi) reducing vulnerability to threats. If we take a look at the worst hoarders, they rank very highly on the GHSI. Out of 195 nations, Canada ranks fifth and the UK ranks second. The highest ranked nation on the GHSI, the US, is also a hoarder: it has purchased enough doses to vaccinate its population 2.6 times over (when it comes to hoarding, the US ranks sixth in the world).
The national stockpiling of medical countermeasures, including vaccines and drug treatments, boosts a country’s score. That is, vaccine nationalism—the hoarding of doses by rich nations—is great for boosting national confidence in rich countries’ arsenal of pandemic tools, but it is terrible for global pandemic control.
What this shows is that the global health security agenda is really about national interests and national security. It sees the nation as the locus of action—the agenda focuses on getting individual nations to strengthen their own security. It prizes national selfishness. And national selfishness is bad for any agenda that has as its aim, the security of the globe’s health. If a disease threat anywhere is a disease threat everywhere, as our global health leaders tell us, then this calls for a truly global effort to equitably distribute medical countermeasures.
The vaccine apartheid that we saw during the 2009 H1N1 pandemic, and now during covid-19, shows us that we need a different way of conceptualizing global health security. We fully support the need to have stockpiles of pandemic vaccines, and to be able to surge both vaccine manufacturing capacity and surge the health workforce during pandemics, but the agenda and the locus of action must go beyond the nation state. Stockpiles should be regional or global, and there should be an agreed upon allocation system to ensure equitable distribution of vaccines to susceptible people across all nations in the event of a pandemic. The global health security agenda, and the metrics supporting it, should stop rewarding rich nations for their selfish behaviour and start prizing international collective action.
Adia Benton Associate Professor, Department of Anthropology, Northwestern University, Evanston, IL, USA.
Maimuna Majumder Faculty, Computational Health Informatics Program, Harvard Medical School and Boston Children’s Hospital, Boston, MA, USA.
Gavin Yamey Professor of Global Health and Public Policy, Center for Policy Impact in Global Health, Duke Global Health Institute, Duke University, Durham, NC, USA.
Competing interests: AB declares that she has no competing interests. MM declares that she has no competing interests. GY declares that he is a signatory to the People’s Vaccine Campaign and is a funding member of Amnesty International, one of the members of the People’s Vaccine Alliance. He was a member of the COVID-19 Vaccine Development Taskforce, hosted by the World Bank, and participated as an academic unpaid adviser in the consultation process that led to the launch of COVAX, a global Covid-19 vaccine sharing mechanism. He has received grant funding from the WHO, Gavi, the Vaccine Alliance, and the Bill & Melinda Gates Foundation.