In our #ebnjc blog series we have already celebrated children’s nursing; with blogs from Jayne Pentin, Kirsten Huby & Marcus Wootton, learning disability nursing; with blogs from Professor Ruth Northway, Jonathan Beebee & Amy Wixey, midwifery; with blogs from Louise Silverton CBE , Gina Novick & Lynsey Wilgaus, and adult nursing from Clare McVeigh, Professor Roger Watson, Professor Jan Dewing & Professor Elizabeth Robb
This week our #ebnjc December blog series concludes with four guest blogs on mental health nursing from Neil Withnell, Jessie McGreevy, Paul Canning & Peter Jones.
Today we welcome Peter Jones, a community mental nurse older adults. In today’s blog Peter discusses the dual legacies of a health career.

The dual legacies of a health career and a baton to match
Legacies are omnipresent. For new students in health and social care being a learner also means picking up the legacies of senior peers. For staff entering the final years of their career, they too may reflect on what for them are career legacies. By this I mean the problems that seem to recur, the issues that innovation, funding, partnership, collaboration, care philosophy, technology and the latest and greatest have failed to solve.
The word ‘legacy’ instantly throws up history. My history spans mental health care from 1977 in the institutions and from 1985 to today community based mental health in several roles. As a student nurse I remember the legacies that we had to avoid picking up. Not just the huge tea-pot for all but the fact that milk and sugar was already added. Pre-lockers, there was the laundry room where shirts and pants could be found for ‘long stay’ patients, but even experienced staff failed to develop a tailor’s eye for instant fit. The theory – practice gap was evident as the director of nurse education did not wish for students to start as nursing assistants: theory must be first? As the calendar flicks from 2015-16 the care delivery debates are various and still include task-centredness vs. person-centeredness vs. service-centred, integrated care and parity of esteem and so on.
These are just a few legacies, the point being that they are actually career legacies in the sense of being pervasive and a facet of the business of caring. In this sense they cannot be ‘solved’. They can be re-solved with whatever contemporary lens we wish to apply. They are there when you start, wet behind the ears, and a humbling reminder as you consider the close of your career. Clearly profound progress has been made especially in mental health. These legacy issues are however a feature of nursing, of healthcare, of medicine; a feature no-less of the human condition that precedes the health focus here. The others include holistic care, not the new-age crystal type but care that considers the person as a whole.
If we cannot really solve these healthcare problems what can we do? The notion of health career provides an avenue. Even if we cannot solve them perhaps there is a positive legacy in some of the tools that history itself can provide. In learning the lessons of history for me this comes in the form of Hodges’ Health Career Model. ‘Career’ refers to the life chances that follow an individual from their epigenetic beginnings, conception through the life course. As ‘model’ suggests there is a structure upon which legacies and much more can be hung and severally examined.
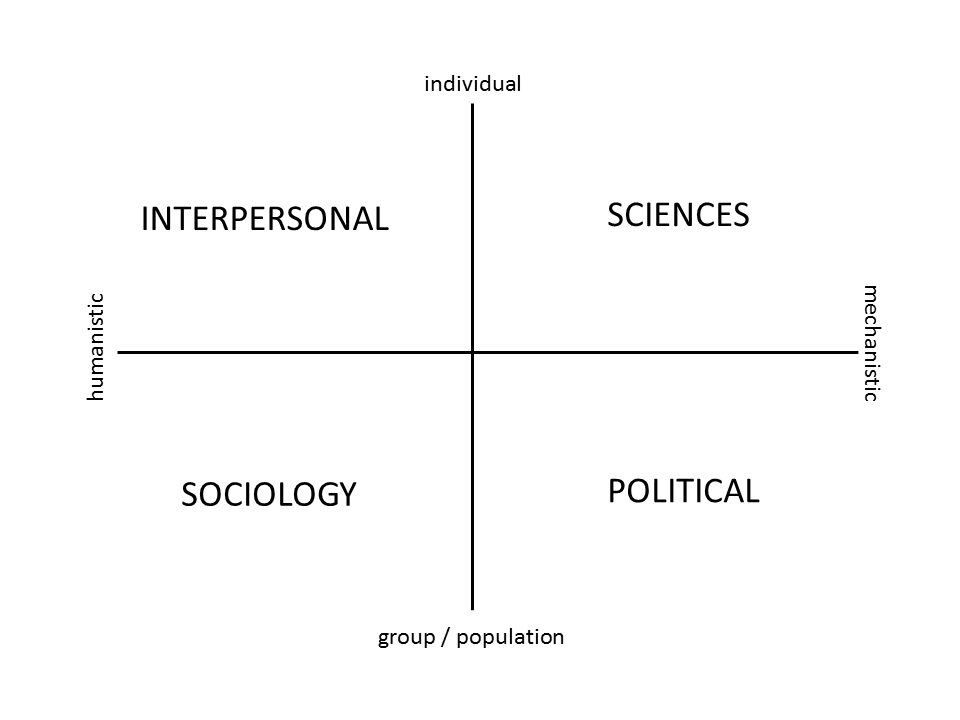
Through Hodges’ model we can help equip new learners with a conceptual framework to quickly appreciate the ramifications of legacies and the current situations they encounter. Then they can conceptually orientate themselves to what is a fascinating, dynamic and rewarding career. A tool to represent, reflect upon and share the features of the healthcare landscape must be evidence-based. Studies are underway to theoretically underpin the model to ensure it is more than a historical artefact. The inclusion of a political domain, as illustrated, makes the model relevant and fit for the 21st century. Certain educational theories, such as, threshold concepts appear to be applicable. Literally picking up the intersecting axes of Hodges’ model as a baton, a student would be given to ask: what is this? This in itself is a good start! We need to assure reflective practice and critical thinking, so essential to address the ongoing legacies that are health and social care.
Biography
Peter Jones RMN, RGN, CPN(Cert.), PGCE, BA(Hons) Comp/Phil, PG(Dip)COPE lives and works in South and West Lancashire as a full-time community mental nurse older adults. Peter has championed Hodges’ model on the web and currently through distance learning studies at Lancaster University in technology enhanced learning. Peter provides a bibliography and blogs about Hodges’ model, informatics, education and health related matters at “Welcome to the QUAD”: http://hodges-model.blogspot.com/
EBN Recommends:
- Kurtz, M. (2013) ‘Cross-sectional study: In individuals with schizophrenia, duration and severity of mental illness, health status, mutuality, employment and household income influence quality of life ‘, Evidence Based Nursing, 16, (3), pp. 79-80
- Gulliver, A. (2015) ‘Cross-sectional study: A range of personality traits and health beliefs influence mental health help-seeking behaviour in young people’, Evidence Based Nursing, 18, (4), pp. 117.
- Haddad, M. (2010) ‘Cross sectional survey: Different attitudes towards mental health revealed in a survey of nurses across five European countries; more positive attitudes found in Portugal, in women and in those in senior roles’, Evidence Based Nursing, 13, (4), pp. 128-129.
- Gaskin, C. and Hardy, S. (2015) ‘The state of play in child and adolescent mental healthcare services (England): not in front of the children?’, Evidence Based Nursing, 18, (3), pp. 1.
- Dr Alison Twycross and Dr Peter Mills Podcast on Self harm within inpatient psychiatric services.