 PrEP—or chemoprophylaxis against HIV infection, as the less sexy phrase goes—is about using chemicals to prevent yourself from contracting HIV during sex or the sharing of injection equipment, the acronym standing for “pre-exposure prophylaxis.” It has gradually emerged as a possibility as a public health intervention after six years of clinical trials. It looks very promising, but only some of the problems that burden it are being discussed during the increasing—and increasingly irrational—hoopla around the topic.
PrEP—or chemoprophylaxis against HIV infection, as the less sexy phrase goes—is about using chemicals to prevent yourself from contracting HIV during sex or the sharing of injection equipment, the acronym standing for “pre-exposure prophylaxis.” It has gradually emerged as a possibility as a public health intervention after six years of clinical trials. It looks very promising, but only some of the problems that burden it are being discussed during the increasing—and increasingly irrational—hoopla around the topic.
The two chemicals in question are emtricitabine and tenofovir, both nucleoside/nucleotide reverse transcriptase inhibitors, combined in the product Truvada, which is used primarily as a medication for treating established HIV infection. That it’s Truvada as opposed to another product is not actually essential to the problems; the chosen drug will no doubt change over time, but Truvada is the exemplar for the moment.
There are usual and unusual concerns. Firstly, does it work? The short answer is yes. That is, in clinical trials. If you use it properly. If it’s part of a comprehensive service of prevention, including regular HIV testing, counselling, condom provision, and the diagnosis and treatment of (other) infections. In other words, it works in just the same way as condoms do in real life.
There has been a variety of studies showing its efficacy. The most effective trials raise questions around reporting on as treated vs. intention to treat (the latter reportedly showing lesser efficacy), as well as about sampling from highest risk populations, where efficacy is therefore inflated owing to high baseline risk, which also reduces one’s ability to extrapolate to a wider population. Still, it would be unwise to attempt to claim that PrEP is not efficacious to some degree. Two more recent, European studies (PROUD and IPERGAY), using very different dosing approaches, have been terminated early owing to clear evidence of efficacy. Yet, as the medical journalist Gus Cairns has noted, the closure of trials of efficacy does not mean that the questions are all answered.
{kind=link}
The primary problem with PrEP is that, firstly, just as with HIV medications and condoms, it would not necessarily be delivered as part of adequate services in the clinic and, secondly, we don’t always use them properly, sometimes for very good reasons. In real life, physicians won’t always be compliant with guidelines that require PrEP to be prescribed as part of even a minimal programme of behavioural health, and this will increase the risk of problems that are already well evidenced with both PrEP and HIV treatment, such as non-adherence and disengagement from services. The “cascade of care” for high risk HIV negatives will abruptly stop there.
The evidence of PrEP’s effectiveness in even the most rigorous epidemiological modelling of PrEP is predicated upon the continuation of the same level of condom use in at risk populations. Jean-Michel Molina, principal investigator of the IPERGAY trial, is reported to have said that “condoms remain the cornerstone of HIV prevention.” Yet, while a great deal of effort is going into promoting PrEP, little is going into promoting other methods or even combined prevention—at the same time as services are doing away with even low competence health advising, in tandem with the rise of over the counter HIV testing kits.
The simple reason for a lack of appropriate delivery within sufficiently comprehensive services is that providing competent behavioural health services is neither what physicians do, nor how they see “medicine,” so it gets sidelined. The chairman of the UK government’s Expert Advisory Group on AIDS (formerly a solely physicians’ committee) stated that behavioural science and behavioural medicine are “window dressing” (I quote). Given that HIV is a behaviourally driven global pandemic, that’s deeply wrong. The sidelining was also evident in the way that, following the introduction of antiretroviral therapy in 1996, the previously patient centred health services were fractionated, outsourced, and dismantled—including behavioural and social health services—in favour of a return to purely physician centred HIV services, which is what we have now. Not coincidentally, transmission rates then began to rise, having been stable previously for a decade.
Physicians being drug therapists and surgeons, behavioural interventions don’t figure among their competencies. A physician expecting that he can provide behavioural interventions competently is like a psychologist assuming he can do surgery. Yet, in my 32 years of receiving services for HIV, I’ve never encountered a clinical health psychologist in a sexual health clinic, let alone a GP’s office. With the roll-out of PrEP, the consequences of this will become ever worse.
It is also very telling that the physicians I speak to don’t even understand what behavioural medicine is, often confusing it with consultation liaison psychiatry. In practical terms, a physician saying “use a condom too” is as effective as the American Christian social health initiative “just say no to drugs.” It’s irrelevant to people’s lived experience and fails to address the mental and social determinants of those behaviours. Such an attitude also bears the odour of medical paternalism, and the evidence resistant belief among physicians that theirs is the only profession ill people need in order to get well and stay well. It hasn’t been true yet—ever—so I’m unsure why we continue to act as though it will be in the future.
Then there is the issue of cost: in the US, PrEP costs about $1500 every month (about £12 000 every year, currently). This is in comparison to the estimated lifetime cost offset (or income loss to the medical industry) of a prevented infection—currently reported to be about $335 000. Yet this does not use a total costs approach, including the potential costs to the individual, such as non-prevented injury from other STIs and other behaviourally driven illnesses that the biotech “quick fix” will leave unaddressed, while spreading the financial cost to other services. Here, a question of clinical negligence arises, not just poor health policy.
Equally, it might be that there is a reduction in risk behaviour associated with PrEP (as suggested by some research), which could be exploited for therapeutic and preventive benefit in services that integrate behavioural medicine—except that there is not a sexual health clinic in the UK that does this (and, no, sexual health advising does not equate). What are the financial and social costs of this omission in reference to PrEP’s potential?
There are also concerns around the physical toxicity of PrEP. It also has interactions with certain antibiotics, antimalarials, anticonvulsant(s), antivirals, cholesterol reducing agents, bone density promoters, and so on. Ten per cent of Truvada users experience diarrhoea, dizziness, headaches, rash, fatigue, and hormonal problems. Who will pay for the consequences of toxicity and the reduced efficacy of combined treatments if it’s part of a public health programme rather than a treatment, or if the person doesn’t have funded access to clinical services free at the point of use?
A lot of the unspoken nature of such problems relates, as usual, to the fact that clinical trials look at the prevention of HIV transmission only, thereby setting the scope of discussion, rather than addressing the larger and more important question of comprehensive health outcomes: does this intervention help people stay healthy and how? Here, “health” is not merely the absence of HIV infection, but its physical, mental, and social aspects, which are mediated by behaviour in its broadest sense and which drive acquisition of chronic illnesses generally, including HIV.
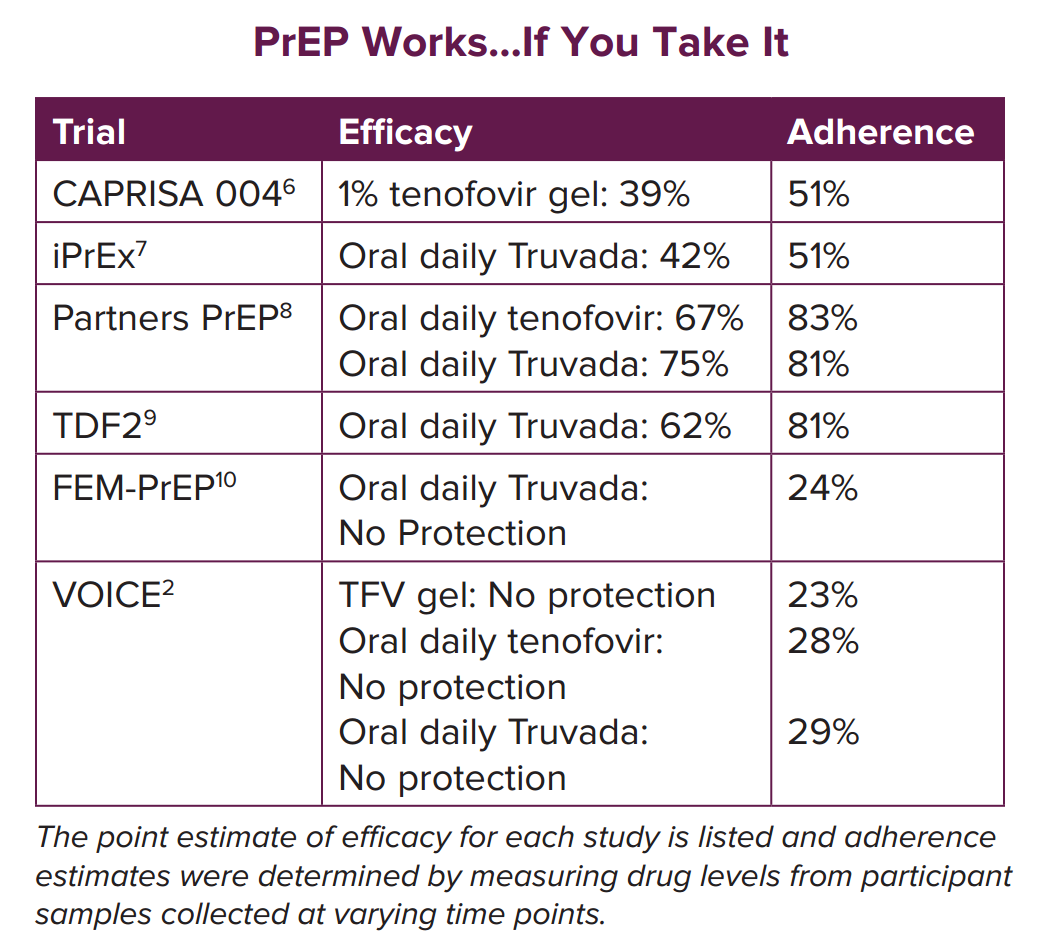
In the PrEP trial with the lowest efficacy, the FemPrEP study in African women, “despite substantial counselling efforts, drug adherence appeared to be low,” indicating that the very same mental and social determinants of HIV transmission are the ones that reduce the utility of PrEP in the communities that need it the most. Ironically, PrEP could also be a tool of empowerment, particularly for women, if used in the right way by the clinics. There will be a need for studies that address these wider issues if we are to answer “is PrEP health effective.”
Furthermore, inadequate monitoring of new infection in someone who has been prescribed PrEP means that there might be the development of drug resistant virus during primary infection. This would make it all the harder to treat, and also increase the risk of that person transmitting drug resistant virus to someone else taking PrEP, thus exacerbating the problems associated with HIV.
While AIDS activism has been attributed as the cause of the movement of global health, PrEP contains all the issues of that field writ small, applying equally to first world health systems. On a group level, the types of risks cited above may (or may not) be relatively small, but for the person who suffers them they are not hypothetical or trivial. This distinction raises the ethical (not to mention medicolegal) problem of the tension between public health and medicine, the former addressing group health and the latter (allegedly) individual health. The two should work together, but that would require, again, integrated and patient centred services, not the physician centred services we have today.
While addressing those issues in HIV is essential, affected communities themselves need to be proactive, in order to protect their rights and fulfil their social responsibilities (whatever they are determined to be). For example, PrEP costs a lot, and we need to address that in terms of both drug rationing and exaggerated concerns about health tourism, which we already have to cope with, as well as criminalisation and immigrant bashing.
Yet, at the 29 September conference of the International Association of Providers of AIDS Care (IAPAC), called “Controlling the HIV Epidemic with Antiretrovirals: Avoiding the Cost of Inaction,” one panel discussant baldly said, “we don’t have time for ethics” (I quote). That perceived lack of time is precisely because we have not taken the time before to consider these applied issues in PrEP fully. We have to start sometime.
AIDS activism can also go wrong, and we are seeing that in the simplistic hype and the sometimes bitterly snide attacks on critics of PrEP’s wider roll-out. At the IAPAC conference, more than one presentation (including physicians’) made statements along the lines of “either you’re with us or you’re against us.” It rings of the evangelical, revival tent crusades, of faith rather than science, and this has no place in public health or medicine. It is also retrogressive advocacy of a 1980s style, but what is most sad is that it is most typically advocacy by activists who have failed to move on from the “more drugs” discourse to one of “more health,” which is a far more complex and intellectually demanding area of advocacy. In a unique form of regulatory capture, such activists have been kept on the treadmill of drug advocacy, failing to address the larger issues.
While PrEP has great potential, that potential is being damaged badly by its own advocates, in their failure to address these larger issues in a manner sufficiently sophisticated to create progressive health policy—policy that serves the needs of the public, not just of physicians, pharmaceutical companies, and the outdated activists they have in their wake. PrEP is not a simple issue and it cannot be reduced to such, no matter the strength of the faith attached to it.
The bottom line is encapsulated by the following questions (and answers): does it work (yes); is it health effective in real life (partially and variably); is it more sexually health effective than condoms in real life (probably not); can it replace condoms (no); can condoms replace it (no—especially with needle sharing); is it necessary (yes, for some people); is it cost effective as a preventive (only for certain, behaviourally targeted individuals); does its real life use promote other illnesses and increase the burden on other services (not yet studied); ethically, should it be prescribed in conjunction with competent behavioural health services (yes); will its prescription occur in conjunction with competent behavioural health services (no); would prescribing it in conjunction with competent behavioural health services increase its specific preventiveness, while also reducing comorbidities and thus service burden and costs (highly likely, but not yet studied).
All the trials to date have shown: 1) it can work extremely well; 2) it doesn’t work unless you address the social, mental, and behavioural determinants of health and illness, particularly among the most needy. Pretending that PrEP solves the behavioural and social issues around risky sex and intravenous drug use is like pretending that there will be a pill for bad housing soon. PrEP is the latest in a long line of hyped fads, which will eventually settle down to taking an important place alongside many others in the large armamentarium of tools and methods used against the HIV pandemic. We need to moderate the hype around PrEP, while at the same time ensuring that the business of physician centred medicine does not proceed as usual, and thereby injure its potential. PrEP is too valuable to allow that to happen.
Rupert Whitaker co-founded, and is now patron of, the Terrence Higgins Trust, as well as chairman of the Tuke Institute, focusing on international health services research and policy. He brings personal experience of disability from HIV and stroke, and 30 years of medical and scientific expertise developing health effective services for patients. He qualified in psychiatry, neurology, and immunology in the United States.
I declare that I have read and understood BMJ policy on declaration of interests and I have no relevant interests to declare.