By Amali U Lokugamage Elizabeth(Liz) Rix, Tania Fleming, Tanvi Khetan, Alice Meredith, and Carolyn Ruth Hastie.
The global pandemic and the BlackLivesMatter movement have highlighted systemic racism as a driver of health inequities for ethnic minorities in the United Kingdom. So how should we upend this pervasive discrimination and critically yet constructively examine this from a decolonial perspective? This collection of authors from the UK, New Zealand and Australia have co-produced a Cultural Safety framework to address structural iatrogenesis where patients are harmed by unconscious or conscious racist power imbalances in the bureaucratic and cultural systems within healthcare systems, including those systems originally intended to help them.
Health inequities are known to be directly linked to colonisation by the British Empire and the enduring legacy of individual and structural racism. Cultural Safety’s genesis was in New Zealand, created and developed in the 1990s by Māori nurse and educator, Irihapiti Ramsden. The shared experiences of all Indigenous Peoples colonised by Europeans have prompted the expansion of the Cultural Safety educational framework to Indigenous Peoples and other marginalised ethnic minority populations globally. The Australian perspective in particular reveals parallels with the UK in the context of both countries’ social and political landscapes, including hidden colonial histories, healthcare inequities and racial discrimination. Whilst the UK context and history of racial discrimination are literally ‘poles’ apart from that experienced by Māori and Aboriginal Peoples in the Antipodes, outcomes for those suffering individual and systemic racism when accessing healthcare resonate strongly.
Cultural Safety differs from other frameworks (such as cultural competence) for developing healthcare practitioners’ cross-cultural skills in a number of crucial areas which we discuss in our article Translating Cultural Safety to the UK. Critical self-reflection on one’s own culture, power, and privilege, and addressing inherent power imbalances within healthcare sets Cultural Safety apart as a decolonising and human rights focused framework. Cultural Safety is also crucial to undoing discrimination and critical conversation about racism in our health institutions. Translating Cultural Safety to the UK therefore is a form of reverse innovation from people who were colonised back to their previous colonisers to address racial injustice in healthcare. This means that the ex-British empire could humbly learn from others who have been subjugated and subordinated about solutions that have arisen and work well from grassroots experts. From this trajectory we can address knowledge/epistemic blind spots in healthcare structures arising from unconscious bias, power imbalances and privilege known to have been set up and ingrained during the origins of biomedicine in colonial times.
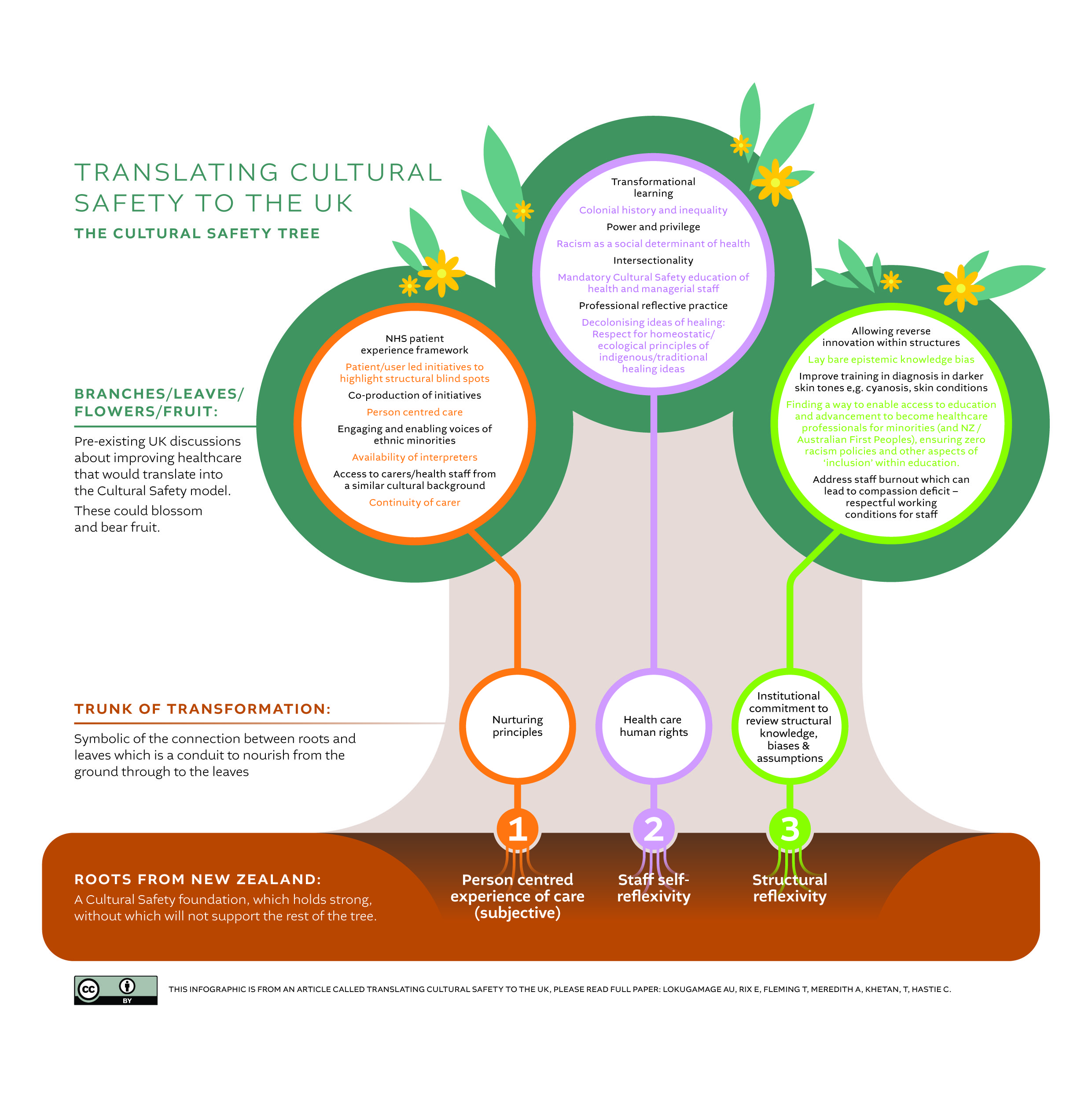
For the translation of Cultural Safety to the UK, we have developed an infographic to assist readers (graphic above). We use a Cultural Safety Tree model as both a practical taxonomy but also as a metaphor which symbolises and resonates with its Indigenous ideals.
Person-centred care, staff reflexivity, structural reflexivity and listening to the voices of the recipients of healthcare are the crucial roots to this model. Organisations can explore the other aspects representing the tree trunk and the multiplicity of possible strategies and actions (representing the flowers, leaves and fruit). We acknowledge that the translation of CS, will require dovetailing and tailoring with pre-existing healthcare human rights, ethics, undoing racism and decolonial activities within the UK. Actively engaging with this model will lead to dismantling the underlying discrimination and unconscious biases that have become embedded as structural racism within policy, systems, and practice. A practical example of this in the context of the UK, is the historical absence of teaching materials for diagnosis in dark skin tones, with resources universally focused on white skins. These omissions are in effect, the vehicles of misdiagnosis and potentially death. A clear and concerning example of this is not teaching medical, midwifery, and nursing students how to diagnose cyanosis in a black person.
Denial of the existence of structural racism in the UK by the recent Sewell report has been condemned and rejected by many experts and contradicts scholarly outputs in this context. The evidence of structural racism is undeniable, despite the Sewell report attempting to shift the focus from racism to geography, family, culture, and religion. Educating healthcare providers to work in a Culturally Safe way in the UK will require further research and policy development. Doing so will provide an important steppingstone in overturning structural racism within the NHS and beyond.
Paper Title: Translating Cultural Safety to the UK
Authors: By Amali U Lokugamage1,2 Elizabeth(Liz) Rix3, Tania Fleming4, Tanvi Khetan5, Alice Meredith5, and Carolyn Ruth Hastie6
Affiliations:
1 Department of Clinical and Professional Practice, University College London Medical
2 School, London, UKDepartment of Women’s Health, Whittington Health NHS Trust, London, UK
3 Faculty of Health, Southern Cross University, Gold Coast Campus, Bilinga, Queensland, Australia
4 School of Midwifery, Auckland University of Technology, Auckland, New Zealand
5 University College London Medical School Alumni, University College London, London, UK
6 Department of Nursing and Midwifery, Griffith University Faculty of Health, Gold Coast, Queensland, Australia
Declaration of interests: AUL is on the Board of Directors of the International MotherBaby Childbirth Organisation and a member of a Patient and Public Voice Partners advisory group within NHS England (which are both voluntary and non-renumerated roles). TF, ER, AM, TK, CH none declared.
Social media accounts
@DocAmali, https://www.linkedin.com/in/amali-lokugamage-64097b43/
@tania_fleming16, https://www.linkedin.com/in/tania-fleming-2b9b82122/
Liz Rix https://www.linkedin.com/in/liz-rix-870b9231/
@CarolynHastie, https://www.linkedin.com/in/carolyn-ruth-hastie-123a8910/