Do you respond to feedback from audits? Do you think you respond in the same way as your colleagues? If not, perhaps feedback should be provided to you and your colleagues in different ways. This is the proposal from Desveaux and colleagues in their Viewpoint about the role of tailoring in audit and feedback (A&F)1.
Precision medicine – a pathway to follow?
There is a scientific and political push towards ‘precision medicine’ approaches in health care2. There are different levels of precision, from ‘stratified medicine’ to ‘targeted therapy’ and ‘deep phenotyping’, with each emphasizing the use of data and feedback loops to identify increasingly precise ‘treatable traits’ and support personalized health care decision-making. The Viewpoint describes an equivalent process within A&F: identifying categories of observable characteristics, developing methods to stratify A&F recipients by these characteristics and tailor feedback accordingly, and predicting and testing a ‘treatment’ response2. Initial characteristics for tailoring feedback and testing responses might be quite broad (e.g. age and gender). Such characteristics provide the opportunity to learn what it is about these characteristics that lead to differences in response to A&F and how to undertake tailoring in subsequent iterations.
Tailoring is broadly defined as a process of designing and adjusting interventions to suit local conditions (see Box). Tailoring is based on the underlying assumption that change is more likely when the intervention and its implementation align with salient factors that influence practice. Such influences are sometimes referred to as determinants, barriers or facilitators.
|
“Tailored interventions to change professional practice are interventions planned following an investigation into the factors that explain current professional practice and any reasons for resisting new practice. These factors […] may vary in different healthcare settings, groups of healthcare professionals, or clinical tasks.”3 |
|---|
Box. What is tailoring?
Tailored interventions have been shown to be effective in improving professional practice and health outcomes, but the effect is variable and tends to be small to moderate3. Tailoring is carried out in many different ways and it is currently not clear what the best approach is and for whom. So, what would it mean in practice to tailor A&F?
What should be tailored and at what stage in the A&F cycle?
To tailor A&F, we would need to understand the patterns of action/inaction following an A&F intervention, which would include identifying the barriers and enablers to enacting such feedback. When gathering information about influences on practice, it is important to consider the extent to which these influences are stable traits or states that vary, for example, over time or between performance measures. To illustrate, consider the feedback a driver gets from the car dashboard: will they react in the same way to a fuel light as to a faulty brake warning light? Such different responses may also occur with different forms of clinical performance feedback; for example, health professionals may react differently to feedback about higher-risk medications (e.g. opiates, insulin, anti-coagulants) than they would to feedback about lower-risk medications. Responses might also vary at different times (e.g. during regulatory visits or after recent safety conferences).
The potential influences on the effectiveness of A&F also may vary depending on the stage of the feedback cycle4. For example, issues may arise during the health professional’s interaction with the feedback, in the course of later sensemaking work to verify and accept the feedback, or while enacting follow-up behaviours intended to improve performance. Fortunately, there are opportunities to tailor A&F to address different barriers and alter the response within each of these stages (Table).
Table. Opportunities to tailor audit and feedback (A&F) at different stages of the feedback cycle
|
Stage in the feedback cycle |
Possibilities for tailoring A&F and/or adding co-interventions to improve response |
|---|---|
|
Goal setting |
|
|
Data collection |
|
|
Feedback |
|
|
Interaction with feedback |
|
|
Sensemaking work to verify and accept the feedback |
|
|
Behaviours intended to improve performance |
|
Tailoring could be undertaken by intervention deliverers, recipients or through co-design involving both. For example, Roos-Blom and colleagues tested an A&F intervention on pain management in the intensive care unit that included a ‘toolbox’ with a pre-determined list of potential barriers and suggested evidence-informed actions5. In this case, earlier work by the intervention providers narrowed the list of potential determinants and proposed linked actions. In other examples of A&F interventions, tailoring work is undertaken by the feedback recipients. For example, Sykes and colleagues organised virtual workshops for the recipients of national audit feedback to allow them to explore local influences on national audit performance and commitment to change, and to identify and enact strategies aligned to those influences6.
To add to the complexity, interventions such as A&F can be tailored at multiple levels to target barriers and enablers at the individual professional, group, or organisational level. Desveaux and colleagues describe opportunities to improve clinician performance by tailoring feedback to both the professional (recipient skills and characteristics) and the organisation (organizational and professional culture and ‘fit’ with existing workflows)1.
Developing a logic model to articulate how the tailored A&F intervention is understood to have its effect may help those designing and delivering A&F to consider the level at which they anticipate the intervention to work and the level(s) at which they should tailor or provide co-interventions. The Figure below provides an example of a high-level logic model for the National Diabetes Audit in the UK7. It suggests there to be national and organisational-level improvement actions that are expected to change health professional behaviour and subsequently patient behaviour. Tools such as logic models, causal pathway diagrams8, and the action-effect method9 can provide a foundation from which to identify the mechanism(s) of action and anticipate influences (pre-conditions or moderators) on that effect, such as the recipient characteristics and cultural context identified by Desveaux.
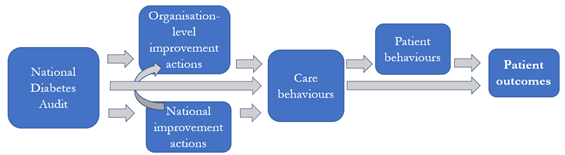
Figure. The levels through which the UK National Diabetes Audit potentially influences patient outcomes7
A&F: an exemplar for tailoring QI interventions
It is easy to become overwhelmed by the number of possible design choices involved in tailoring of A&F interventions. However, there is also a number of reasons for using A&F as the quality improvement intervention upon which to extend our understanding of tailoring:
- A&F is a commonly used improvement strategy (e.g. approximately 60 national audits in England alone10), presenting the opportunity for testing different design choices at scale
- A&F is a much-tested intervention (e.g. 293 trials of A&F have been identified11)
- There is an international collaboration between researchers and audit providers exploring ways to systematically test different designs (see https://www.ohri.ca/auditfeedback/ 12)
- There are prioritised theory-informed hypotheses describing potential enhancements to A&F13
- There are methods through which to facilitate discussions with stakeholders and articulate how a strategy such as A&F leads to proximal and distal outcomes (e.g.8,9)
- There is a growing evidence-base investigating the conceptualisation, application and effect of tailoring 14,15
Coming back to our original question, maybe you don’t respond to performance feedback in the same way as your colleague, but providing different feedback to you both could lead to the same intention to change. Identifying ways to tailor feedback to create that intention represents a potential (and testable) advancement for A&F. The authors point to Google, Netflix, and Amazon as examples of interfaces that are personalised to the recipient based on artificial intelligence. Tailoring is used at present within some local electronic health records, often manually (e.g. practices adding electronic prompts). Providing health professionals with the capability to tailor feedback reports and dashboards may provide a window of opportunity to learn about the determinant–content couplings and inform more automated approaches. Such individual level approaches would need to complemented with tailored strategies to address organisation- and national-level influences on A&F.
–Dr. Sheena McHugh & Dr. Michael Sykes
Dr. Sheena McHugh (@SheMcHugh) is a Senior Lecturer and health services researcher at the School of Public Health at University College Cork and an Associate Editor at BMJ Quality & Safety. Her primary research interests are implementation science, quality improvement, and chronic disease management. Dr. Michael Sykes (@Msykes09) is a Senior Research Fellow in the Department of Nursing, Midwifery & Health at Northumbria University. His research seeks to enhance the organisational response to audit and feedback.
References
1. Desveaux L, Rosenberg-Yunger ZRS, Ivers N. You can lead clinicians to water, but you can’t make them drink: the role of tailoring in clinical performance feedback to improve care quality. BMJ Qual Saf. Published Online First: 12 December 2022. doi: 10.1136/bmjqs-2022-015149.
2. König IR, Fuchs O, Hansen G, et al. What is precision medicine? Eur Respir J. 2017;50:1700391. doi:10.1183/13993003.00391-2017.
3. Baker R, Camosso-Stefinovic J, Gillies C, et al. Tailored interventions to address determinants of practice. Cochrane Database Syst Rev. 2015;:Cd005470. doi:10.1002/14651858.CD005470.pub3.
4. Brown B, Gude WT, Blakeman T, et al. Clinical Performance Feedback Intervention Theory (CP-FIT): a new theory for designing, implementing, and evaluating feedback in health care based on a systematic review and meta-synthesis of qualitative research. Implement Sci. 2019;14:40. doi:10.1186/s13012-019-0883-5.
5. Roos-Blom M-J, Gude WT, de Jonge E, et al. Impact of audit and feedback with action implementation toolbox on improving ICU pain management: cluster-randomised controlled trial. BMJ Qual Saf. 2019;28:1007-15. doi:10.1136/bmjqs-2019-009588.
6. Sykes M, O’Halloran E, Mahon L, et al. Enhancing national audit through addressing the quality improvement capabilities of feedback recipients: a multi-phase intervention development study. Pilot Feasibility Stud. 2022;8:143. doi:10.1186/s40814-022-01099-9.
7. Sykes M, Berry A, Colling S, et al. Report on the National Diabetes Audit (NDA) Quality Improvement Collaboratives. London: 2020.
8. Lewis CC, Klasnja P, Powell BJ, et al. From Classification to Causality: Advancing Understanding of Mechanisms of Change in Implementation Science. Front Public Heal. 2018;6:136. doi:10.3389/fpubh.2018.00136
9. Reed JE, McNicholas C, Woodcock T, et al. Designing quality improvement initiatives: the action effect method, a structured approach to identifying and articulating programme theory. doi:10.1136/bmjqs.
10. Foy R, Skrypak M, Alderson S, et al. Quality Improvement: Revitalising audit and feedback to improve patient care. BMJ. 2020;368. doi:10.1136/BMJ.M213.
11. Grimshaw JM, Ivers N, Linklater S, et al. Reinvigorating stagnant science: implementation laboratories and a meta-laboratory to efficiently advance the science of audit and feedback. BMJ Qual Saf. 2019;28:416. doi:10.1136/BMJQS-2018-008355.
12.Ivers N. Updating the Cochrane audit and feedback review-completing a decade long odyssey. 2022; Ottawa Health Research Institute, Canada. Available from https://www.ohri.ca/auditfeedback/af-metalab-conference-2022/
13. Colquhoun HL, Carroll K, Eva KW, et al. Informing the research agenda for optimizing audit and feedback interventions: results of a prioritization exercise. BMC Med Res Methodol. 2021;21:20. doi:10.1186/s12874-020-01195-5.
14. Riordan F, Kerins C, Pallin N, et al. Characterising processes and outcomes of tailoring implementation strategies in healthcare: a protocol for a scoping review. HRB Open Res. 2022;5:17. doi:10.12688/hrbopenres.13507.2.
15. Wensing M. The Tailored Implementation in Chronic Diseases (TICD) project: introduction and main findings. Implement Sci. 2017;12:5. doi:10.1186/s13012-016-0536-x.