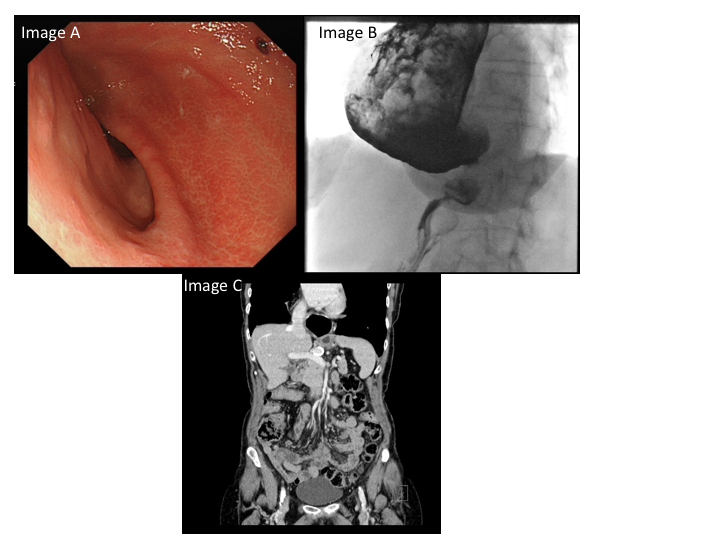
A 78-year old lady with a previous history of oesophagectomy for adenocarcinoma, was referred with symptoms of epigastric pain, post-prandial vomiting and weight loss. OGD after a prolonged fast revealed erosions in the gastric conduit (image A) and the impression of external indentation at the antrum but no stenoses. Biopsies revealed chronic inflammation with no evidence of dysplasia or malignancy. A barium meal and CT abdomen were ordered and the results are shown in image B and C respectively.
What is the cause of gastric outflow obstruction?
Dr Isabel Carberry 1, Dr Jim Zhong 2, Dr Nick E Burr 1, Dr Damian JM Tolan 2
and Dr Venkat Subramanian 1
Leeds Gastroenterology Institute, Leeds Teaching Hospitals NHS trust, Leeds, United Kingdom 1
Department of Clinical Radiology, St James’s University Hospital, Leeds Teaching Hospitals NHS trust, Leeds, United Kingdom 2
Corresponding author
Dr Venkataraman Subramanian
Leeds Gastroenterology Institute, Leeds Teaching Hospitals NHS Trust, Beckett Street, Leeds, LS9 7TF
v.subramanian@leeds.ac.uk
Answer:
The OGD and barium meal showed a dilated gastric conduit with large amounts of food residue. There was transient hold-up of contrast caused by extrinsic compression of the first part of the duodenum by a 2cm, rim-calcified mass. The subsequent CT scan showed a heavily calcified common hepatic artery aneurysm (HAA) which indented the pylorus and was the cause of her gastric outlet obstruction.
HAA are rare and asymptomatic in 75% of patients. Unfortunately, around 15% of patients present with a rupture.[1] In symptomatic patients, epigastric pain and jaundice are the most common features.[2] HAA are more frequent in males, associated with hypertension, smoking and alcohol intake, malignancy[1] and previous biliary surgery.[2] When suspected CT angiography can characterise the lesion and inform future treatment decisions which can include stenting, embolisation, ligation and vascular reconstruction.[2]
We could not find any other reports of HAA causing gastric outlet obstruction, although a case involving a pancreaticoduodenal artery aneurysm has been described.[3] Although rare, visceral artery aneurysms should be recognised in the aetiology of gastric outlet obstruction. Our patient’s symptoms have eased with conservative management including dietary modification and proton pump inhibitor therapy. She is awaiting a review by the local surgical MDT.