In mid-July 2024, Fatima gave birth to her first child in a town in South Kordofan. Just a day later, paramilitary forces attacked her town, forcing her to flee to a remote village without healthcare. In August 2024, famine was declared in the same region she fled. Fatima’s child is now nearly one year old and has never received any vaccine due to a lack of access to routine immunisation services.
Meanwhile, another mother remains trapped in El Fasher—the historical capital of Darfur—besieged since April 2024 by the Rapid Support Forces, a non-state armed group. She lost her husband to indiscriminate shelling, and the city’s only maternity hospital, run by a non-government organisation, has been under attack and partially destroyed. Her third child received only a single dose of the polio vaccine before the siege, leaving him under-vaccinated for two years.
These stories and many others were drawn from the daily realities of ongoing conflict situations faced by millions of families and their children, not only in Sudan but across various conflict-affected settings worldwide. Children born during ongoing or protracted conflicts are often reported as either unvaccinated or under-vaccinated, reflecting a broader public health crisis that affects vulnerable populations globally.
While many children still get sick or die because of conflicts, vaccines have prevented about 154 million deaths, including 146 million children under five and 101 million infants under one, since 1974. Vaccines are essential tools in saving children’s lives, especially during conflicts. When accessible, they effectively prevent vaccine-preventable diseases, which are among the leading non-violent causes of death among children in such crises and can serve as a gateway to provide other public health services through integration.
The recent annual WHO/UNICEF national immunisation coverage (WUENIC) report details global vaccination uptake in 2024, focusing on the first and third doses of Diphtheria-Tetanus-Pertussis (DTP) and the first and second doses of measles vaccine coverage. Published in mid-July, the report reveals that the number of zero-dose children—defined as those who did not receive any DTP dose—and under-vaccinated children still exceed pre-COVID-19 pandemic levels and are not on track to reach a 50% reduction in zero-doses by 2030, which is one of the key impact goal indicators in the Immunization Agenda 2030 (IA2030). The report also showed that 51% of these unvaccinated children are residing in countries with fragile, conflict, and vulnerable settings. According to the report, Sudan has the lowest DTP vaccination rates globally (48%) and ranked fifth lowest countries with measles vaccination (46%), highlighting the urgent need for humanitarian corridors to supply public health services, including vaccination.
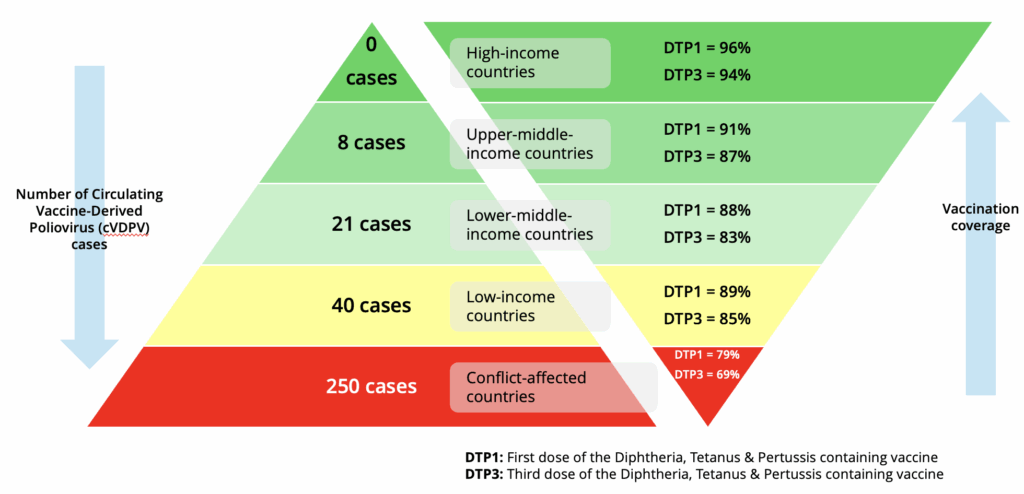
In this article, we further highlight the global equity gap in vaccination coverage and polio cases between conflict-affected and non-conflict-affected countries. We introduced a new diagram using WUENIC data from 2024 to emphasise and clearly illustrate that children who reside in these conflict-affected settings continue to be left behind. Our analysis focused on first and third dose Diphtheria-Tetanus-Pertussis (DTP) vaccine coverage and circulating Vaccine-Derived Poliovirus (cVDPV) across conflict-affected countries, as well as in countries with varying income levels—high, upper-middle, lower-middle, and low income. The results, showing number of polio cases and vaccination coverage, are depicted in two layered pyramids inspired by Maslow’s hierarchy of needs (Figure 1), with the base representing essential human needs necessary for survival. In public health terms, this corresponds to access to basic vaccines.
The cVDPV cases signal failures of early vaccination milestones, which include DTP and polio vaccines. The form of polio vaccines differs by country, but they are co-administered with DTP vaccines. DTP coverage serves as a proxy indicator for polio vaccination. We included countries with WUENIC estimates using WHO dashboards: 21 conflict-affected and 167 non-conflict-affected countries, including 61 high-income, 49 upper-middle, 44 lower-middle, and 13 low-income countries. Conflict-affected countries are those with high insecurity due to active or protracted conflicts, as listed annually by the World Bank. The 2024-2025 list comprises 21 countries, half in Africa. The list includes 15 low-income, five lower-middle, and two upper-middle income countries.
The first pyramid shows global cVDPV cases. Twelve conflict-affected countries reported 250 cases, representing 78% of global cases—over six times the number of cases in non-conflict-affected low-income countries (40) and no cases reported in high-income countries. The corresponding second pyramid shows DTP1 and DTP3 coverage from 94% and 96% in high-income countries and 79% and 69% in conflict-affected countries.
These trends of inequity in polio vaccination coverage and disease burden, including cVDPV, have persisted in conflict settings, and our diagram (Figure 1) clearly demonstrates that children who reside in these settings continue to be left behind, remaining at the bottom of the hierarchy even in 2024. This depicts a disproportionate disease burden and stark inequity in access to immunisation.
In 2023, 85% of children affected by polio lived in fragile and conflict-affected countries. The Global Eradication Polio (GPEI) identified in 2023 ‘‘most consequential geographies,’’ which accounted for 90% of all new polio cases worldwide. These areas include eastern Afghanistan, southern Khyber Pakhtunkhwa in Pakistan, Tete province and nearby regions in northern Mozambique, eastern Democratic Republic of Congo, northern Yemen, northern Nigeria, and south-central Somalia- all characterised by high populations of zero-dose children and under-vaccination. In 2024 alone, Afghanistan and Pakistan reported 25 and 74 wild polio cases, respectively.
Many structural challenges in conflict-affected settings impact the delivery of childhood vaccines, including polio. These include lack of access to communities by national immunisation programs and humanitarian actors, intensified in territories controlled by non-state armed groups, such as extremist groups in the Sahel region, where violence against health workers is increasing. Similarly, protracted conflicts have intensified mistrust, including questioning the motives of international actors, hampering efforts to eradicate polio.
Recent cuts to global development assistance risk further marginalising children who are already at the bottom of this pyramid. Vaccine equity is critical if we are to deliver on the Immunization Agenda 2030 to protect all children from vaccine-preventable disease.
Authors:
Majdi M. Sabahelzain, Research fellow at the Sydney School of Public Health and Sydney Infectious Diseases Institute, Faculty of Medicine and Health, University of Sydney, Australia.
Harriet Dwyer, PhD student at the London School of Hygiene and Tropical Medicine in the UK.
Penelope Robinson, Senior Research Officer at the Sydney School of Public Health, Faculty of Medicine and Health, University of Sydney, Australia.
Meru Sheel, an Associate Professor and applied epidemiologist at the School of Public Health, Faculty of Medicine and Health, University of Sydney, Australia.
Julie Leask, Professor and social scientist at the School of Public Health, Faculty of Medicine and Health, University of Sydney, Australia.
Conflicts of interest:The authors declare the following financial interests/personal relationships, which may be considered as potential competing interests: Julie Leask has received travel support for an overseas meeting from Sanofi in 2024. All other authors state that they have no conflicts of interest, financial or personal, that might have influenced the work reported in this paper.
Handling Editor: Neha Faruqui