Self-managed abortion, or abortion self-care, is when a pregnant person obtains an abortion without supervision by a healthcare professional.
Safe abortion self-care requires:
- Access to accurate information on the dosing, timing, how to manage pain, and when to seek further help;
- Access to medicines of reliable quality;
- Confirmation of success, and options for contraception.
Abortions, miscarriages and births at home have a long history as part of ancestral and Indigenous birthing practices. The process of colonisation has led to the imposition of Western medical models of maternal healthcare globally, and has privileged Western research over Indigenous ways of knowing and being. Through the forced displacement of Native American nations, in-depth connection and knowledge of botanical remedies to assist in commonplace medical needs, developed over centuries, has been lost
“We knew what kind of plants were available, how to use them, and how to harvest them. We used them in lactation, headaches, indigestion and abortion” says Rachael Lorenzo, who is of the Mescalero Apache, Laguna Pueblo and Xicana tribes and is current Co-Executive Director of Indigenous Women Rising, a reproductive sovereignty organization that provides financial assistance to Native abortion seekers in the USA. They explain that Western colonialist frameworks often value a live birth above all else. In contrast, the Indigenous worldview centers the wellbeing of the collective, regardless of birth outcome. The ritual ceremony of burying remains on tribal lands is the same whether the pregnancy loss was due to induced or spontaneous abortion.
Globally, the legal status of abortion self-care varies, with self-management often criminalised even in countries like the UK, where abortion access is assumed. Indigenous practices of abortion, rooted in autonomy and community, stand in stark contrast to these state-imposed controls.
The legal and structural barriers to self-managed abortion perpetuate settler-colonial oppression while denying Native peoples their inherent right to practice traditional birthing. To continue to deny Native people the ability to practice and preserve their languages, cultures and traditions in light of the violent and genocidal history is unconscionable.
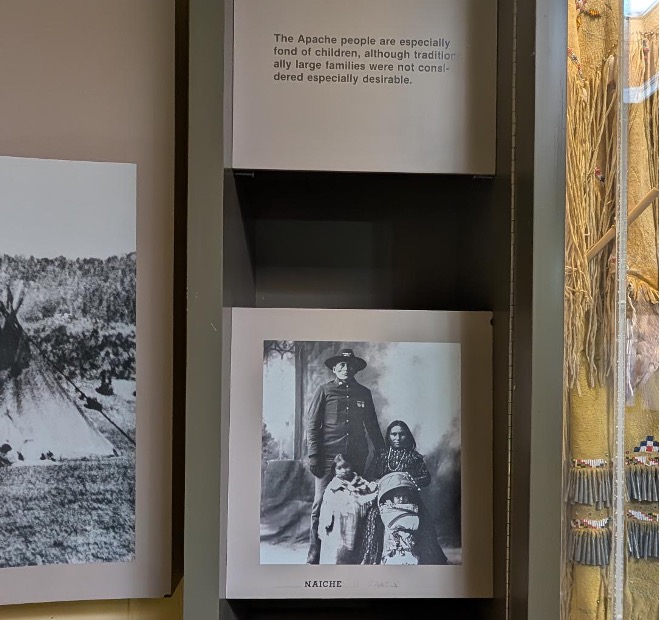
Lorenzo shares a photograph from the Mescalero Apache Tribe Museum in New Mexico, showing a mother, father, and two children, a small glimpse into the Apache’s nomadic life. Without permanent settlements and facing threats like warfare and drought, families had to constantly assess the safety of each pregnancy. In this context, abortion was necessary for the wellbeing of the entire family unit, including the pregnant person and the fetus.
“Menstrual regulation” is the term used for when a menstrual period is missed, and techniques including use of abortifacients are used to induce menstruation whether or not pregnancy is confirmed. It is a well-documented, commonplace traditional practice in many cultures globally.
Mohawk midwife and Indigenous feminist Katsi Cook links the movement for sovereignty of “Land Back” to sovereignty over Indigenous bodies. Indeed, the universal principle of bodily autonomy can be applied as an argument for availability of self-managed abortion for all. “What is good for Native people is good for everyone” is a quote attributed to Tecumseh, a Shawnee warrior and chief in the late 1700s and early 1800s. This idea still resonates today, where global healthcare inequalities continue to exist along racial lines. Homebirth, midwife-led birth, doulas and use of non-medical therapies such as massage, peer-support, and hypnobirthing have well documented, evidence-based benefits in maternal care. However due to structures that hegemonizes capitalism, patriarchy and Western models of healthcare delivery, these forms of care are often unavailable both in high and low-income settings. The global trend we see now is one of medicalization of birth and increase in operative birth without a clear and proven benefit. Instead, linked to increased medical interventions and lack of bodily autonomy in birth, we have growing concerns around birth trauma and poor maternal mental health.
A modern vision for what self-managed abortion may look like, that respects traditional knowledge and cultural safety, as well as incorporates our current evidence-base for safe abortion care, calls for a decolonization approach. Steps and strategies to achieve this include:
- Decriminalization of abortion as the global minimum standard
- De-regulation of use of medication abortion in the first trimester. There is currently work being done on the safety and usability of over-the-counter mifepristone-misoprostol combipacks. The challenge lies not in creating a safe, user friendly product for abortion seekers, but in overcoming societal and legislative stigma around abortion.
- Ensuring recourse to non-medical and medical support during the abortion process and in post-abortion care. Self-managed abortion is not “abortion alone”, and its safe and acceptable practice relies on the presence of accompaniment or other facilitators of accurate information including digital tools, helplines, as well as recourse to medical support if needed or desired.
Author: Dr Sabrina Das was born in Singapore to migrant parents and identifies as a multiracial (Sri-Lankan/Indian/Chinese), Brown-bodied woman. She is an Obstetrician and Gynaecologist and 2024-25 UK Harkness Fellow hosted at the CUNY Graduate School of Public Health.
Acknowledgements for editorial input for this article to:
Rachael Lorenzo, Co-Executive Director for Indigenous Women Rising (Mescalero/Apache/Laguna Pueblo/Xicana tribes);
Janell Dymus-Kurei, 2024–25 Aotearoa New Zealand Harkness Fellow in Health Care Policy and Practice Director of Tauukiuki, an Indigenous Sovereignty Organisation (Te Whakatōhea).
Competing interest: None
Handling Editor: Neha Faruqui