WHO declared COVID-19 as Global Pandemic on March 12, 2020, at present, it is devasting entire World with 5691,790 cases and 355,629 deaths [1]. India reported the first case of COVID-19 in end of January 2020, and total reported cases crossed 1,58,000 cases with 4,534 deaths on May 27, 2020. COVID-19 is primarily transmitted through respiratory droplets, and non-pharmaceutical interventions are the only tool to suppress the disease [2,3]. Almost 66% of the population lives in rural parts of India. However, a large majority of cases of COVID-19 in India are concentrated in a few cities. Congested urban areas provide a scope of rapid transmission to COVID-19 in India, as observed in other countries. We observe that predominantly urban distribution of the disease with high population density and high prevalence of comorbidities.
We retrieved COVID-19 data from covid19india.org, a crowdsourced platform for COVID-19 data in India. Data for the urban population, population density, and population above 60 years was extrapolated for 2020, using the Census of India 2001 and 2011. District level prevalence of diabetes, hypertension, obesity, adult anemia, in 15-54 years age group and the number of individuals slept in a room in the household were calculated using data from National and Family Health Survey of India (2015-16) [4,5].
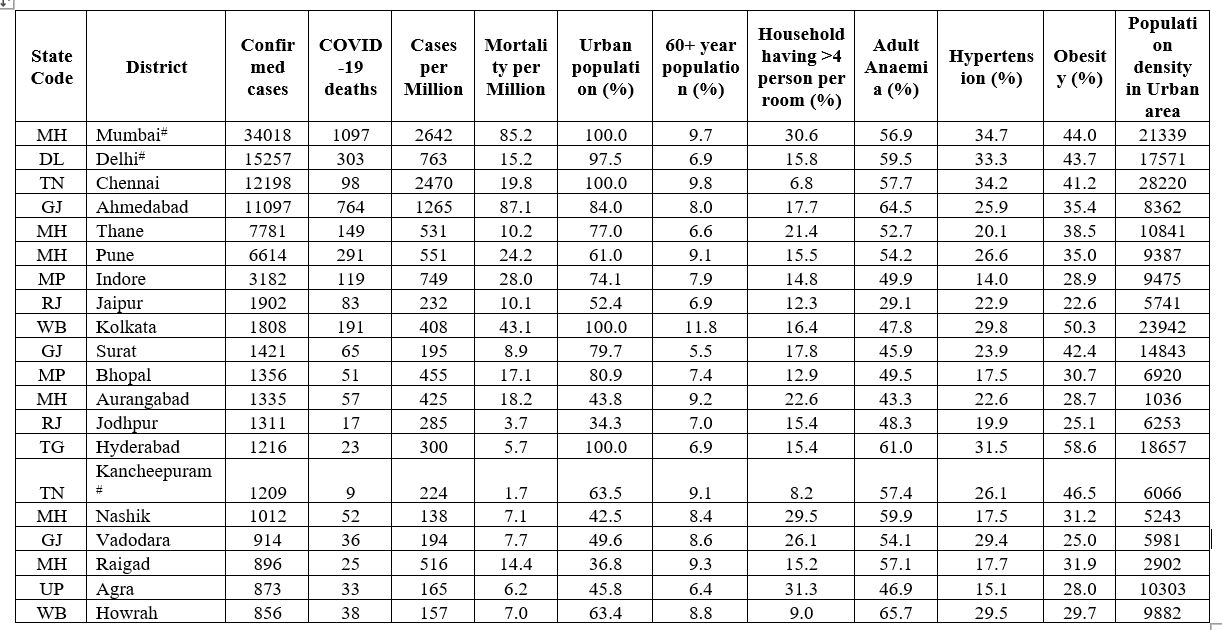
We observed that 67.2% of cases of COVID-19 and 77.2% mortality related to COVID-19 are concentrated in only 20 districts (2.7%) out of a total of 739 districts of India. These 20 districts have only 10.5% of the 1.35 billion total population of India. We also observed 50.8% cases, and 53.2% of deaths of COVID-19 are concentrated in only five cities of India: Mumbai, Delhi, Ahmedabad, Chennai, and Thane having only 4.4% of the Indian population. All cities having the highest burden of COVID-19 either have an International airport or are major financial/tourist hubs, with a population density of 1,036-28,220 persons per square Kilometre (KM) in urban areas. All the major COVID-19 hotspot districts are urban, and 15 out of 20 districts have more than 50% urban population.
Editorial Note : BMJ Global Health Blogs is not peer-reviewed.
Note: Mumbai and Mumbai suburban are merged in COVID-19 reporting, we followed same for other characteristics. We considered Delhi as a place only for analysis because districts were not mentioned for Delhi COVID-19 data. Kancheepuram district was bifurcated in Chengalpattu and Kanchipuram in 2019, we used undivided Kancheepuram district information.
Mumbai has the highest burden of COVID-19 cases and more than 31% households of Mumbai reported more than four individuals sleeping in a single room. Apart from COVID-19 prevalence, death per million population is a good indicator to measure health system response, containment measures and overall management of COVID-19 [6]. In India, COVID-19 national death per million (DPM) is 3.4, it places India in a good position in comparison of Belgium (805 DPM), Italy and United Kingdom (545 DPM), France (437 DPM) and many other countries. Total 130 countries have death per million more than Indian average [7]. However, death per million, in ten out of top 20 districts is higher than national average and maximum in mega cities like Ahmedabad (87 DPM) and Mumbai (85 DPM), which is more than 25 times of national average. It may reflect that few cities have COVID-19 burden completely different from rest of the country.
Without any vaccine/treatment for COVID-19, non-pharmaceutical interventions are only measures to control the COVID-19 epidemic. However, in crowded large cities, it is challenging to maintain one-meter physical distance due to lack of proper space within and outside the home. We find that very few districts with large cities are having an overwhelmingly large proportion of COVID-19 cases in the country. In our analysis, high urban proportion and population density were significantly correlated with the COVID-19 burden in districts having the highest burden of COVID-19. It seems COVID-19 is spreading only in a limited number of large cities/districts with high population density. A tiny proportion of the cases are in rural areas or small cities and towns. Similar findings were reported in another study [8]. Indian districts are large, with about 65% of Indian districts have more than one million population. At present, only district-level data is available. It gives only a very gross picture of the districts as well as country. Declaring an entire district as a Red zone (high case burden) or Orange ( moderate case burden), and locking down the whole district may risk other health services as well as closing all social and economic activities will have major financial burden [9]. We argue that the availability of more granular data at the ward level in cities and sub-district level in the rural area,together with ;ocal policy flexibility at a lower administrative level, might help achieve better control. It is the right time to focus on a robust public health system to manage COVID-19 and to prepare for any future pandemic as well as to achieve sustainable development goals [10].
Editorial Note : BMJ Global Health Blogs is not peer-reviewed.
About the authors:
Ashish Awasthi is Assistant Professor, Biostatistics at Centre for Chronic Conditions and Injuries, Public Health Foundation of India. He is an INSPIRE Faculty supported by Department of Science and Technology, Government of India, New Delhi. He tweets @AwasthiAshish15
Dileep Mavlankar has been heading the Indian Institute of Public Health Gandhinagar as its Director since 2012. He is the Chair of Technical Working Group on Maternal Health by Government of India and a member of the Steering Group on Health for the 12th Five-year Plan of the Planning Commission of India. He tweets at @DMavalankar
Competing Interests
We have read and understood the BMJ Group policy on declaration of interests and declare the none interests.
Acknowledgment:
Ashish Awasthi is supported by Department of Science and Technology, Government of India, New Delhi through INSPIRE Faculty Program, for some other work.
References:
1 CSSE. COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE) at Johns Hopkins University. https://coronavirus.jhu.edu/map.html
2 Lewnard JA, Lo NC. Scientific and ethical basis for social-distancing interventions against COVID-19. Lancet Infect Dis 2020.
3 World Health Organization. Modes of transmission of virus causing COVID-19: implications for IPC precaution recommendations: scientific brief, 27 March 2020. World Health Organization 2020.
4 Dubey M, Rastogi S, Awasthi A. Hypertension prevalence as a function of different guidelines, India. Bull World Health Organ 2019;97:799–809. doi:10.2471/BLT.19.234500
5 Prenissl J, Jaacks LM, Mohan V, et al. Variation in health system performance for managing diabetes among states in India: a cross-sectional study of individuals aged 15 to 49 years. BMC Med 2019;17:92. doi:10.1186/s12916-019-1325-6
6 Deaths Per Million Key Indicator Of COVID Containment & Case Management. https://www.indiaspend.com/deaths-per-million-key-indicator-of-covid-containment-case-management/
7 Total confirmed COVID-19 deaths per million people, May 26, 2020. 2020.https://ourworldindata.org/grapher/total-covid-deaths-per-million
8 Rocklöv J, Sjödin H. High population densities catalyse the spread of COVID-19. J Travel Med 2020;27. doi:10.1093/jtm/taaa038
9 Adepoju P. Tuberculosis and HIV responses threatened by COVID-19. Lancet HIV 2020;7:e319–20.
10 Panda BK, Kumar G, Awasthi A. District level inequality in reproductive, maternal, neonatal and child health coverage in India. BMC Public Health 2020;20:58. doi:10.1186/s12889-020-8151-9