Eosinophilic oesophagitis (EoE) is an allergic disease of the oesophagus characterised by an elevated eosinophil count on oesophageal biopsy. It classically presents with dysphagia in adults; symptoms in children can be more varied, including abdominal pain and vomiting as well as dysphagia [1].
It is a relative newcomer in the world of gastrointestinal disease, first having been described just over 30 years ago, but its incidence is increasing, even taking into account increased knowledge of the condition and better diagnostic strategies [2].
In this #FGblog we want to draw Frontline Gastroenterology readers’ attention to two recent open access papers published in the journal on EoE; one offering insights into the real-world experience of EoE in England, and the other ways in which care for patients living with this condition can be improved.
Xu et al. integrated and interrogated three national databases to evaluate EoE-related symptoms and comorbidities in 2381 patients with EoE compared to 9365 age and sex matched controls [3]. As might be expected, patients were predominantly male (70.1%) and young (median age 40). 29.2% of patients with EoE had one or more allergic comorbidity, the most common being asthma.
Some of the more hard-hitting findings include the fact that 15.5% of patients had a diagnosis made 24-36 months after symptom onset. Factors associated with this prolonged time to diagnosis included having symptoms of acid reflux or heartburn, which would fit with symptoms being attributed to gastro-oesophageal reflux disease rather than EoE, but interestingly also with age less than 18 years old, and the presence of one or more EoE-related comorbidities. The latter finding is surprising, as the association of EoE with other allergic conditions has been known for a long time.
8.2% of patients presented with food bolus impaction, and 18.3% of patients developed strictures. Although this is the minority of patients, when the ground-level burden on patients and resource use is considered (e.g. emergency endoscopy, therapeutic dilatation), the impact of this ‘rare’ condition is huge.
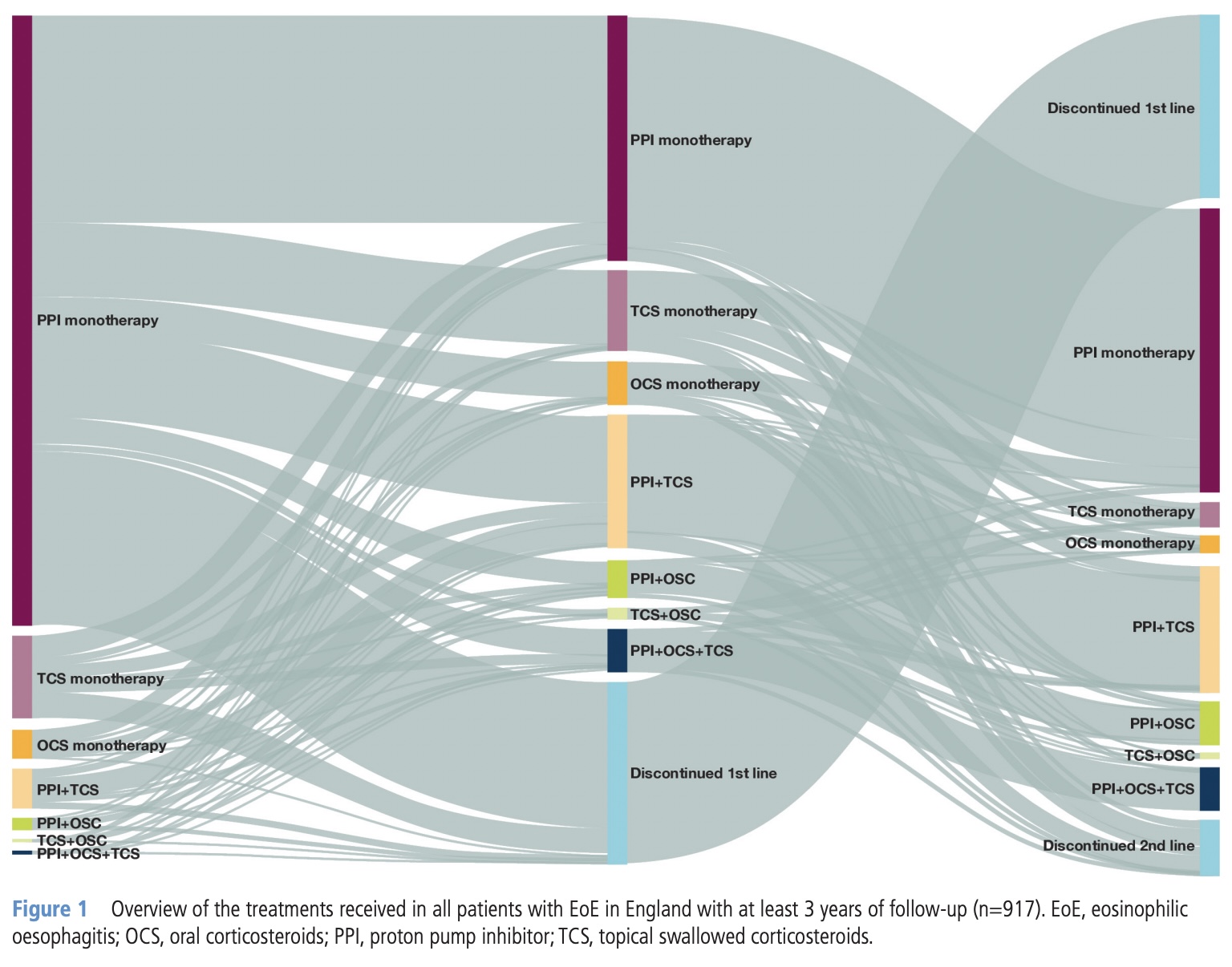
In terms of treatment, most received proton pump inhibitor (PPI) monotherapy as first line therapy, and if patients were switched, the most popular alternative was PPI with topical corticosteroid (TCS).
The pathway agreed on in two expert group meetings are clear, evidence based, and will be for many, practice-changing. Out for good are non-recommended medical therapies for relieving food bolus obstruction such as buscopan, glucagon and Coca Cola (other ineffective fizzy drinks available). In are recommended time intervals to OGD of within 6 hours, 24 hours, or 2 weeks depending on whether the patient is distressed, stable but at risk of aspiration, or if the food bolus has passed respectively. More on recent advances in EoE can be found here [5].
The need for multiple oesophageal biopsies to increase diagnostic yield should be standard practice; the authors recommend at least six biopsies from multiple sites, ideally three. The diagnostic threshold recommended is >15 eosinophils per 0.3mm2 of oesophageal epithelium.
First line medical therapy for induction of remission is unequivocally budesonide orodispersible tablet (ODT). PPIs and dietary interventions usually fail and result in more repeat endoscopies, and compliance with the strictest, more effective six-food elimination diet is low.
Patients should also be on maintenance treatment once remission is achieved as relapse rates following treatment cessation are high. Once again, the best option is budesonide ODT, which is both effective and safe in achieving clinico-histological remission.
We would strongly encourage readers to read the full versions of both of these excellent papers, which are certainly cause for reflection on the care we provide to people living with EoE.
References
- Shillitoe B, Lee JC, Hussien M, et al. Clinical spectrum of paediatric and adult eosinophilic oesophagitis in the North East of England from 2016 to 2019. Frontline Gastroenterology 2022;13:231-236. https://fg.bmj.com/content/13/3/231
- Dhar A, Haboubi H, Auth M, et al. Eosinophilic oesophagitis: improving diagnosis and therapy – reducing the burden of repeated endoscopy. Frontline Gastroenterology 2022;13:e51-e56. https://fg.bmj.com/content/13/e1/e51
- Xu X, Chen SY, Maslova E, et al. Clinical symptoms, comorbidities, treatment patterns and time to diagnosis in patients with eosinophilic oesophagitis in England: a retrospective cohort study. Frontline Gastroenterology Published Online First: 08 August 2024. doi: 10.1136/flgastro-2024-102646 https://fg.bmj.com/content/early/2024/08/08/flgastro-2024-102646
- Dhar A, Attwood S, Basu K, et al. Improving management of eosinophilic oesophagitis in adults in the UK: proposal for an integrated care pathway. Frontline Gastroenterology Published Online First: 12 August 2024. doi: 10.1136/flgastro-2024-102768. https://fg.bmj.com/content/early/2024/08/11/flgastro-2024-102768
- Attwood S, Epstein J. Eosinophilic oesophagitis: recent advances and practical management. Frontline Gastroenterology 2021;12:644-649. https://fg.bmj.com/content/12/7/644
Author: Dr James Kennedy (Trainee Associate Editor)
Twitter: @DrJMKennedy
Declarations: I am a trainee associate editor for Frontline Gastroenterology