It’s not a secret. I have a sub-specialty interest in inflammatory bowel disease (IBD). I like all things IBD- the large patient variation from young to old, the large compendium of medications to trial, the close interaction with the surgeons, the endoscopy assessment and surveillance, the nutritional aspect and the incredible array of research studies available for patients to partake in. In my opinion, IBD is so wide and wonderful, that it’s really a specialty of its own.
Recently, on Twitter, I came across this info-graphic from @drtifftaft on IBD and post-traumatic stress disorder (PTSD):
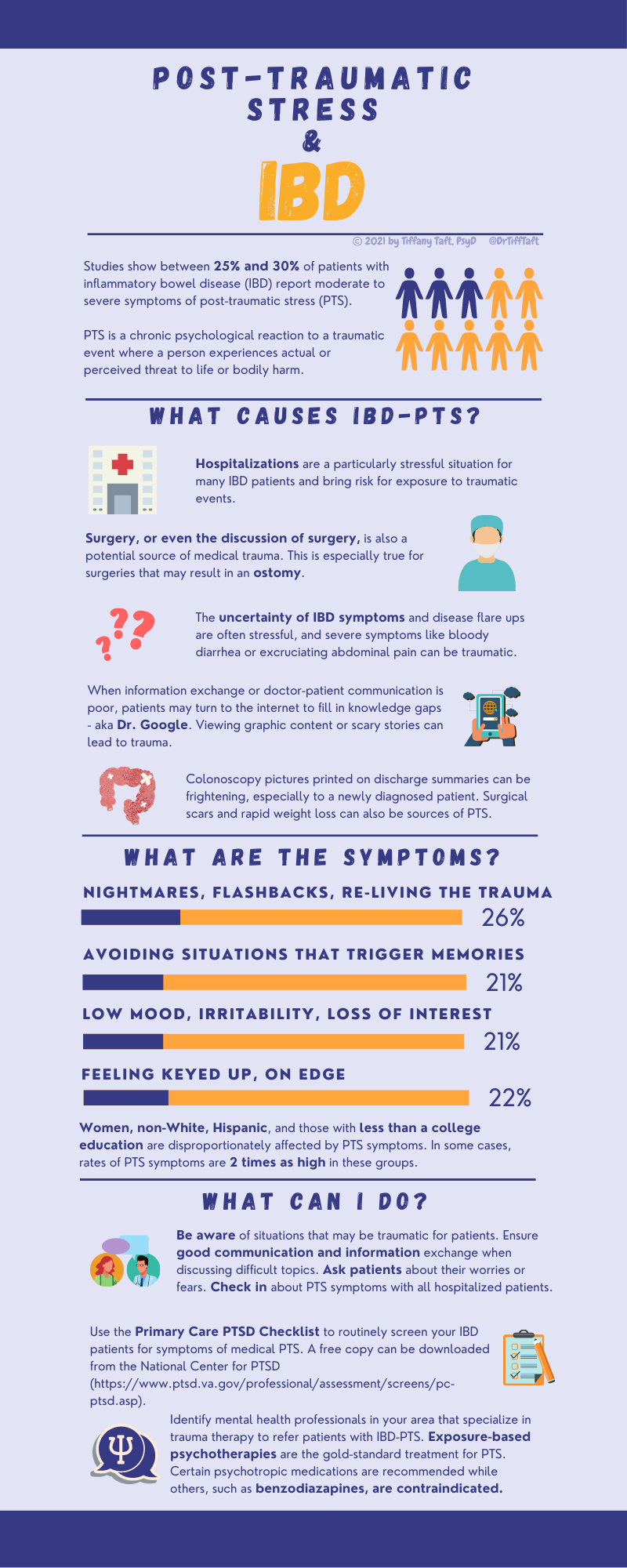
And it started me thinking about IBD and mental health. It’s well known that IBD is associated with mental health problems, particularly depression and anxiety but I had never really associated IBD with PTSD.
I then came upon this paper in Frontline Gastroenterology on “Managing intestinal failure in inflammatory bowel disease- when the drugs don’t work”. The paper itself is highly informative giving a great overview of the aetiology, complications and management of intestinal failure in IBD. However, what really got my attention was the section on psychological support and the risk of PTSD in patients undergoing parenteral nutrition. The paper raises some very alarming points:
- The prevalence of depression in IBD is approximately 15% and 20% for anxiety disorders, which can have a negative influence on IBD and increased relapse rates
- One study demonstrated that of 25 patients who underwent intestinal transplant, ONLY 3 patients did NOT suffer with a psychological diagnosis post-transplant
- Only 34% of patients returned to work after being commenced on HPN (In the IBD cohort, 92.3% were in work prior to HPN initiation which fell to 38.5% after commencement)
I don’t think we take enough time with our patients to talk about mental health and the incredible impact it can have them. So, what can we do as clinicians to help our patients?
- AWARENESS: Be aware of situations that may be traumatic for patients (hospitalisation, surgery, medication changes, need for parenteral or enteral nutrition)
- ACKNOWLEDGE: Ask patients how they are feeling, their fears and concerns.
- REFER: Identify mental health professionals in your area that specialises in trauma therapy and refer early
Clinics can be busy and stressful, particularly trying to keep on time when you’ve already had a late start and likely to go past lunch. It can be very easy to brush off a patient’s mood and ask them to liaise with the GP for further assessment but sometimes patients need that extra 5 minutes to listen to their fears, discuss their concerns and provide reassurance where we can. We need to remind ourselves that mental health is just as important as physical health to maintain remission in our IBD patients.
References: