By Florence Anam1, Cecilia Chung2, Teresia Otieno3, Martha Tholanah4, Alice Welbourn5
As the 23rd international AIDS conference nears, we reflect once more on what it takes to ensure that issues facing women living with HIV are adequately addressed, especially in the context of COVID-19 and increased rates of domestic violence globally. We know how violence increases women’s vulnerability to HIV by 1.5 and worsens its effects: but will the conference, and other authoritative institutions like journals, publishers, and funders, address this?
SRHR of Women living with HIV: New Best Practice
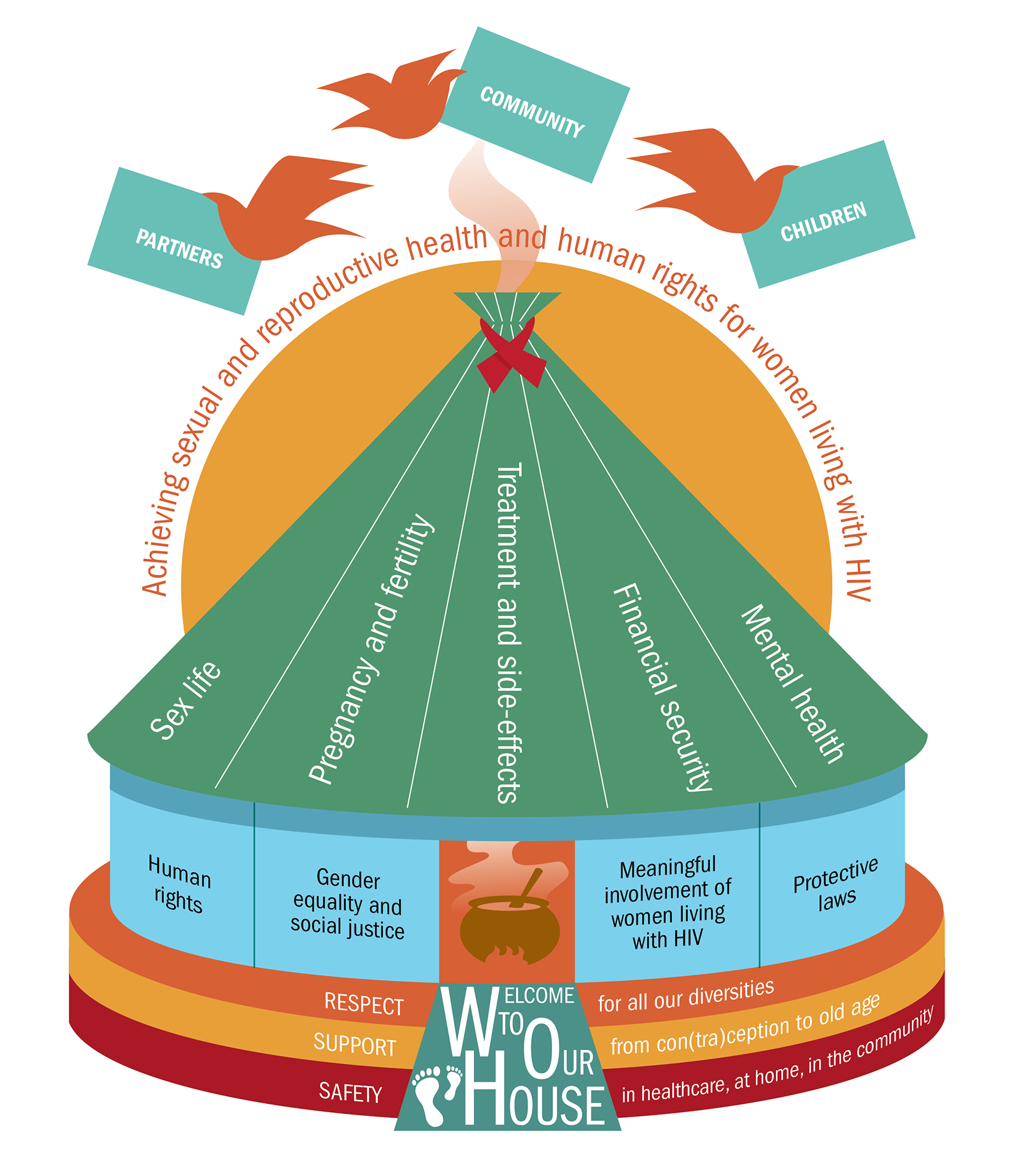
In 2017, the World Health Organisation (WHO) published its latest Consolidated Guideline on the sexual and reproductive health and rights (SRHR) of women living with HIV. A document referenced throughout this Guideline was a global values and preferences study, conducted by, with and for women living with HIV (figure 1), which was commissioned to inform the new Guideline; and violence against women is also highlighted as a recurring theme throughout the Guideline as a result.
Dr Tedros hailed this guideline development process, stating “The process that was followed for the development of this guideline is an approach that we hope can be replicated elsewhere as a best practice for the Organization. This approach further reflects WHO’s commitment to a more person-centred approach and is an enabling initiative that has the potential to support delivery of tangible and lasting public health impact to achieve universal health coverage and improve wellbeing for all.” (pers.comm. August 2017)
One critical guideline recommendation is the meaningful involvement of women living with HIV in all our diversities[1] in research that affects their lives:
“Research about women living with HIV should be conducted with, by and for women living with HIV, as equal research partners. Research that is pursued and funded in this area should include justification for why it is important to women living with HIV.” (6.2.1)
At last! We were delighted to see this recommendation in a global policy document. Our meaningful involvement in research is both an intrinsic right, and a logical necessity, in order to produce policies and programmes which more closely align with and address women’s lived experiences. We thought the world would change.
Business as Usual
How naïve we were. Business has continued as usual with the very people whose lives matter excluded from conversations, and powerless to effect change. This means that the international AIDS conferences still have minimal input from women living with HIV as speakers or co-authors.
This means that in 2018, many women living with HIV faced a crisis, with a sudden blanket ban on dolutegravir in many countries for all women of child-bearing age, with no exceptions, even for those women happily stabilised on the drug who had no plans or chance of getting pregnant.
This means that global organisations continue to fund and conduct operational HIV research without meaningful inclusion of women living with HIV as research partners and co-authors, despite claiming to engage “key stakeholders”.
And most researchers continue to submit top-down biomedical articles about their research ‘in’ or ‘on’ women to journals, using inappropriate language, and no meaningful ‘patient’/ public involvement [PPI]. Furthermore, these articles are written as if those of us living with HIV exist in a political vacuum: there is no consideration, or even acknowledgement, of the critical role of women’s rights organisations in independent movement building for an effective lasting response to violence against women. Yet as the WHO Guideline spells out, violence is a key related factor which has affected so many of our lives.
Leadership from Women living with HIV
In response, we developed an implementation ‘checklist”, to support women living with HIV to work alongside relevant government officials in their countries, to align and tailor their own national HIV strategic plans with and to the new WHO Guideline. The pilot of this in Kenya, funded by UNAIDS was a success. Its pilot extension to some counties by Women Fighting AIDS in Kenya (WOFAK) was also a success. Some of us then documented this, and other women’s inspiring actions elsewhere, in the WHO Guideline (Web Annex 3). This demonstrates how women’s leadership in advancing our rights around the world has improved our sexual and reproductive health, rights and well-being, as well as enabling government health and other staff to understand and respond better to the gaps.
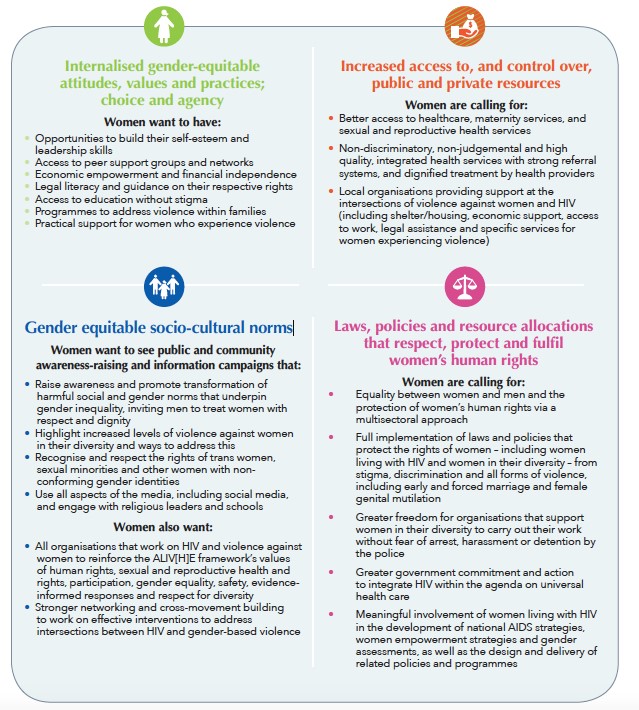
Women regularly fall into these gaps: between countries’ policies and services and what women actually need and want. With further support from UNAIDS, we have developed a participatory peer research approach to addressing violence against women in the context of HIV through a process we have called the ALIV[H]E framework. Here too, we documented how women can be involved meaningfully in research processes; and how this meaningful involvement produces rich information and evidence, based on lived experiences, which can shape policies and programmes to advance and uphold women’s rights and promote more effective strategic use of funding (figure 2). As the WHO Guideline emphasises, research has to go beyond a researcher’s career or the Research Assessment Exercise and have impact in the world.
Despite all our efforts however, we still see scant change. It is time for journals to take a stand to support us, through their editorial and review policies.
Changes in Publishing
As Boivin et al stated in the BMJ: “A second important finding is that the effectiveness of PPI is strongest when people with lived experience of the condition being studied are involved as research partners. This supports the view of patients and the public as experience-based experts who contribute knowledge that is complementary to that of scientists and professionals.”
Survivors’ Voices has produced a checklist for meaningful involvement of women who survive violence in all research that affects their lives. We commend this checklist, which is just as relevant to women living with HIV, to be adopted by the BMJ across all its journals, and by all other leading health journals. It could be a minimal requirement for authors and reviewers to report whether those who seek to have their works published have meaningfully involved the intended ‘beneficiaries’ of knowledge using this checklist. It could be used alongside PRISMA or COREQ as a basic requirement of article submission.
This move by editors could shift goal posts in ways that women living with HIV have long called for but have little power to implement. COVID-19 has shown us what can change when those in power want it to. Journals have the power to shift researchers’ practices and to make huge differences in our lives in the process.
Currently trending political issues such as #metoo and #blacklivesmatter have not just popped up out of nowhere. The causes that drive them have long been deeply relevant to the lives of women living with HIV around the world, whose voices and priorities continue to be silenced or ignored, despite all our best efforts. Systemic and institutional prejudices and responses make differences between rates of survival and death between groups of people.
Whilst the BMJ has had a PPI statement for some time, it could now be advanced by ensuring that researchers who have not involved ‘patients’ in their studies identify this as a clear limitation to their research and list it as an important part of their future research. Readers may say that funds are needed to do this and this is not their responsibility: but publishers such as the BMJ have the potency to change the way researchers, conferences, funders, clinicians and organisations do business. In this way, researchers who want to publish their work may be forced, for a change, to step outside their comfort zones to re-examine current practice, adhere to the evidence base and do what’s right for women’s sexual and reproductive health and rights globally.
We have been calling for our experiences to be prioritised for nearly 30 years, when women living with HIV stormed the stage at the Amsterdam AIDS conference in 1992 and the International Community of Women living with HIV was formed. When will change happen? If research continues not to be directed towards responding to women’s lived experiences and our priorities, we are left asking who are the real key stakeholder ‘beneficiaries’ here?
Fig 1. The ‘safe house’ image from our global values and preferences study on the SRHR of women living with HIV, identifies key priority areas which deeply concern us, which are rarely addressed holistically – or at all – in research.
Fig. 2. This ‘gender change matrix’ shows one example of how women living with HIV and our priorities can be more meaningfully involved in research.
Author Affiliations
1 Médecins sans Frontières; 2 Transgender Law Center; 3 ATHENA Network; 4 Making Waves Network; 5 Salamander Trust.
Notes
[1] By ‘women living with HIV in all our diversities’, we emphasise the fact that we are often considered as a homogenous identity. However, we celebrate our diversities in using this phrase and these include women who are sex workers, women who use substances, women who identify as lesbian, bisexual and trans women, all of whom are sometimes referred to as women from ‘key populations’. We also include Indigenous women, women with disabilities, adolescent girls and young women, post-menopausal women, migrant women, women in minority ethnic groups and women in all corners of the world. These intersectionalities of women’s lived experiences in different contexts adversely affect our vulnerability to and experience of HIV, and should therefore always be taken into account in research, policy and programming.