The release of NICE guidelines allows MESH to be used in the NHS once again; the guidance, however, has proved controversial: MPs and campaigners have warned NICE guidance neglects the serious risks associated with the use of mesh in surgery. They also fear the evidence is untrustworthy, biased and too low quality to inform decision making.
Carl Heneghan
On Tuesday the 2nd April, The National Institute for Health and Care Excellence (NICE) published updated clinical guidelines: Urinary incontinence and pelvic organ prolapse in women: management. [NICE guideline NG123]
This updated guidance comes after NICE, in December 2017, recommended that mesh for pelvic organ prolapse (POP) should be restricted to research only: ‘current evidence on the safety of the procedure shows there are serious, but well-recognised safety concerns’ reported NICE. In September 2018, Scotland’s health boards were ordered to immediately halt the use of mesh implants by the Health Secretary. And in July 2018, The Independent Medicines and Medical Devices Safety (IMMDS) Review, chaired by Baroness Cumberlege, released a statement for an immediate pause in the use of surgical mesh for the treatment of stress urinary incontinence, after meeting women adversely affected by surgical mesh procedures.
This reinstatement of mesh might surprise many; but the vaginal mesh high vigilance restriction period set out in the IMMDS statement was clear that once NICE guidelines on the use of mesh were published, a national register is in place, and specialist removal centres are available then the ban should be lifted:
‘A pause in the use of vaginally inserted mesh to treat prolapse and synthetic tape/sling used to treat stress urinary incontinence will be implemented through a high vigilance programme of restricted practice. This is not a blanket ban; for some patients, this is a debilitating condition for whom a delay or alternative treatment would not be appropriate. Operations will, therefore, be available under the high vigilance programme for carefully selected patients who understand the potential risks.’ (see IMMDS statement)
The NICE guidance states mesh surgery is still subject to a period of “high vigilance restriction” – a term I haven’t come across before and one I couldn’t find any other examples of. The question remains, though, whether there are reasonable reassurances of safety to allow an informed decision to use mesh and whether there is a change in the evidence to justify lifting the ban, particularly the long-term complication rates, where most of the contentious issues are.
NICE state for all mesh procedures ’there is limited evidence on the long-term adverse effects. In particular, the true prevalence of long-term complications is unknown.’ I’ll repeat that – unknown.
This is concerning: as the exposure gets longer the risk of a serious problem – such as mesh exposure – increases. So an examination of the long term complications in NICE’s evidence review is warranted:
Pelvic organ prolapse a total of 81 studies were identified and included: 46 provided data on short-term complications of POP surgery; 24 for mid-term complications and 17 on long-term complications. The 17 studies (3 RCTs, 14 cohorts) were judged to be very low-quality evidence. In total, there were 44 instances of very low-quality evidence mentioned across the evidence review. Only one instance of high-quality evidence was reported.
POP with SUI there were 4 articles reporting data from 3 RCTs (n = 379) included in the review. Because of the low quality and lack of evidence the committee recommended that it is essential to explain to women the gap in the evidence about longer-term outcomes.
Stress Urinary Incontinence found 141 studies and reported on 109 RCTs on the clinical effectiveness and short- and medium-term complications of surgery. There were 259 instances of very low-quality evidence across the statements and only one high-quality evidence statement in 1 RCT (n=179).
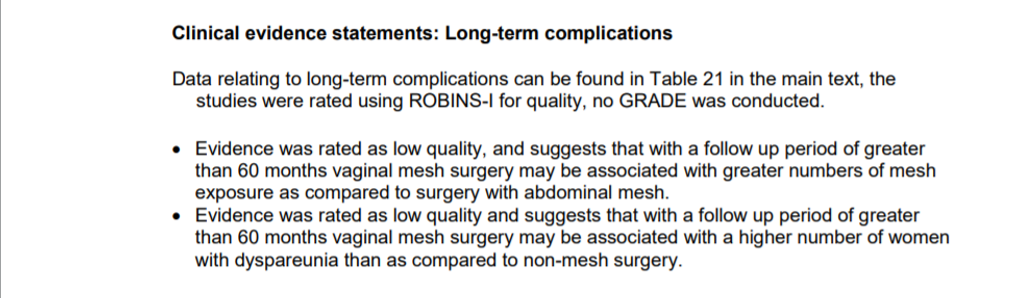
The majority of studies on long-term complications (n=41) were case series (very low-quality evidence), had no comparator groups, and all were judged to be at serious risk of bias (meaning there is considerable uncertainty about whether the complication rates are correct). The complications rates were calculated as weighted averages (see Table 12 and 13 in the evidence review).
Management of complications: The committee also acknowledged the lack of evidence on the management of vaginal complications, sexual dysfunction and/or pain, urinary complications, bowel complications, and general mesh complications in women with SUI, POP or both. A systematic review of the clinical literature was conducted, but no studies were found applicable to the assessment of mesh complications following pelvic floor mesh surgery.
National registry
NICE also recommended that women having surgery for SUI and POP, or who have experienced complications related to surgery, should be asked for their consent to enter their data into a national registry, which should report nationally and each woman should be given a copy of her data.
Research recommendations
The long-term risks of mesh surgery are unknown; there is little – and often no – evidence on complications over the long term, and the quality of evidence is very poor.
NICE’s committee discussed making research only recommendation for POP. However, they considered it would be doubtful that any suggested research would be conducted, as it would be inappropriate to blindly randomise women to mesh surgery. This I find puzzling: surgery is virtually always open-label and not blinded. The way to get around this, and to minimise bias, is to use objective outcomes and to ensure other aspects of the trials (such as the outcome assessors) are blinded.
The committee, also, considered there would be a reluctance to conduct clinical trials because of the controversial nature of mesh surgery, and recruitment would prove difficult because of the potential risks of mesh surgery. Yet, this Is the very reason to conduct research.
The committee believed the long-term effectiveness and harm data would be available from the planned NHS registry. If the registry aims to address uncertainties, then questions should be asked – to an ethics committee – if the registry purpose is one of research.
Registries have traditionally been generated by researchers to collect observational data for a research agenda. They can also be used for audit purposes, to assess care and outcomes against explicit known criteria, or for supporting quality improvement, benchmarking and clinical decision support.
Research occurs, however, when there are unanswered questions that require the collection of data to establish new facts and reach new conclusions. Nothing has changed in addressing the complication rates of mesh in the last 2 years. The purpose of the registry – if I understand it right – is to resolve uncertainties over the long-term complication rates. To be part of the registry is therefore to be part of a research agenda.
Conclusions
Twenty years after mesh was first introduced there are still considerable shortcomings in the evidence base: the quality of evidence for complication is weak and mostly lacking. Given that NICE discarded the NHS Digital review as unhelpful, what is needed is an acceptance that the registry is designed to address important gaps in the evidence – and is, therefore, part of a research agenda.
A registry of all those who have had mesh inserted might be a better idea, and go some way to reducing the current uncertainties about the long term complications.
Carl Heneghan
Editor in Chief BMJ EBM, Professor of EBM, University of Oxford
Competing interests
Carl has received expenses and fees for his media work including from BBC Inside Health. He holds grant funding from the NIHR, the NIHR School of Primary Care Research, The NIHR Oxford BRC and the WHO. He has also received income from the publication of a series of toolkit books. CEBM jointly runs the EvidenceLive Conference with the BMJ and the Overdiagnosis Conference with some international partners which are based on a non-profit model.
DISCLAIMER
The views and opinions expressed on this site are solely those of the original authors. They do not necessarily represent the views of the BMJ and should not be used to replace medical advice. All information on this blog is for general information, is not peer-reviewed, requires checking with original sources and should not be used to make any decisions about healthcare. No responsibility for its accuracy and correctness is assumed by us, and we disclaim all liability and responsibility arising from any reliance placed on such commentary or content by any user or visitor to the Website, or by anyone who may be informed of any of its content. Any reliance you place on the material posted on this site is therefore strictly at your own risk.
’